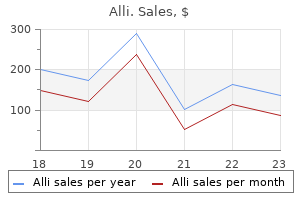
Alli dosages: 60 mg
Alli packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Order 60 mg alli visa
Chronic inactive plaques have more distinctly outlined borders and are grayish in shade with scarred and excavated weight loss 50 lbs quality alli 60 mg, depressed centers (15-6) weight loss katy tx order 60 mg alli mastercard. It is the most typical chronic nontraumatic neurologic disease among younger and middle-aged folks in the developed world. Perivascular persistent inflammation and scattered stellate reactive astrocytes are current. Caucasians of Northern European descent residing in temperate zones are essentially the most commonly affected ethnic group. Clinical presentation varies with heterogeneous neurologic manifestations, evolution, and disability. The interplay between inflammatory and neurodegenerative processes typically leads to intermittent neurologic disturbances followed by progressive accumulation of disabilities. Attacks ("relapses" or "exacerbations") are followed by periods of partial or full restoration. Approximately one-third have an initial episode adopted by regular or near-normal perform. Although most are small-between 5 and 10 mm-large lesions can attain a quantity of centimeters in diameter. Enlarged ventricles and sulci with white matter quantity loss and a thinned corpus callosum are typical findings. T1 hyperintensity is an unbiased predictor of atrophy, disability, and advancing illness. A faint, poorly delineated peripheral rim of gentle hyperintensity secondary to lipid peroxidation and macrophage infiltration typically surrounds sharply delineated hypointense "black holes. Chronic and severe cases usually show average quantity loss and generalized atrophy. Larger lesions often reveal a really hyperintense middle surrounded by a slightly less hyperintense peripheral space (15-15B) and variable amounts of perilesional edema. Note triangle shape and perpendicular orientation of lesions following the course of deep medullary veins. A prominent incomplete rim ("horseshoe") of enhancement with the "open" nonenhancing segment dealing with the cortex may be present, particularly in large "tumefactive" lesions (15-16) (1517) (15-18). Leptomeningeal enhancement occurs in some instances and may be a surrogate marker for cortical demyelination. Steroid administration considerably reduces lesion enhancement and conspicuity and may render some lesions virtually invisible. Myoinositol levels are elevated in acute lesions and are also elevated in normal-appearing white matter. Volume loss with a quantity of hypointense ovoid and triangular lesions within the deep periventricular white matter is current. The broad bases of the triangles are oriented towards the ventricular floor with the apices pointing towards the cortex. Note triangle-shaped occipital lesions with broad bases at the ventricular surface. The left parietal lesion with incomplete ("horseshoe") rim enhancement exhibits diffusion restriction in the periphery surrounding a nonrestricting hypointense core. The left hemisphere lesions show a extra hypointense middle surrounded by a less hypointense rim. The giant left frontal lesion has a very hyperintense middle surrounded by a skinny hypointense rim and peripheral edema. Note that, compared with the size of the lesion, the mass impact is relatively minor. Marked lymphocytic infiltrates (15-19) with inflammatory modifications within the perivenular areas (15-20) result in acute, sometimes fulminant demyelination (15-21). Vasculitis typically preferentially entails the basal ganglia and spares the callososeptal interface. Lesions in Susac syndrome preferentially involve the middle of the corpus callosum, not the callososeptal interface. Rim enhancement-often the incomplete or "open ring" pattern-is seen through the acute inflammatory stage. Signs of increased intracranial strain, aphasia, and behavioral symptoms are typical. Large plaques with alternating rims of demyelination and myelin preservation give the lesion its attribute look (15-23). The F:M ratio is roughly 2:1 and is most typical in sufferers of east Asian origin. Infection, Inflammation, and Demyelinating Diseases 464 demyelinating layers improve on T1 C+ sequences (15-24A). White matter lesions usually predominate, however basal ganglia Demyelinating and Inflammatory Diseases involvement is seen in practically half of all instances. Viral and streptococcal infections have been implicated and trigger enlarged hyperintense basal ganglia, caudate nuclei, and internal/external capsules. Large "tumefactive" lesions cause a gray-pink white matter discoloration and often lengthen all the means in which to the cortex-white matter junction (15-25). Symptoms usually occur a few days to a quantity of weeks following antigenic challenge. However, the illness generally follows an atypical course, waxing and waning over a period of several months. More than half of all patients get well completely inside 1 or 2 months after onset, whereas roughly 20% experience some residual useful impairment. Biopsy disclosed acute demyelinating illness with out evidence of neoplasm or an infection. The typical gross look is that of marked brain swelling with diffuse confluent and/or petechial hemorrhages (15-31A). Hemorrhages are usually present in the leptomeninges, cerebral hemispheres (predominately the white matter), and cerebellum. The massive arteries are regular with out evidence for aneurysm or subarachnoid bleeding. History of a viral prodrome or flu-like illness is widespread however not invariably present. Cross reactivity between myelin fundamental protein moieties and various infectious agent antigens in all probability causes an acute autoimmune-mediated demyelination. Fever and lethargy with rising somnolence, decreased mental standing, impaired consciousness, and longtract indicators are the commonest medical signs. Rapid medical deterioration and death usually occur within days to every week Pathology Location. Basal ganglia involvement is frequent, but the cortical gray matter is usually (but not invariably) spared. Aggressive remedy with intravenous high-dose corticosteroids, immunoglobulin, cyclophosphamide, and plasmapheresis has been used with some success in a quantity of circumstances. Multifocal scattered or confluent hyperintensities as well as bilateral confluent hyperintensity of the cerebral white matter are typical however nonspecific findings (15-32).
Discount alli 60 mg free shipping
This ought to really feel like a bony elevation just medial and posterior to the maxillary tuberosity weight loss zucchini recipes alli 60 mg cheap mastercard. For � � patients with unrepaired clefts of the palate weight loss pills 832 discount alli 60 mg without a prescription, this incision ought to be placed approximately 2 mm lateral to the cleft margin. Incise the left lateral incision from the hamulus to the sting of the hard palate within the midline. Separate the clefted muscular tissues off of the bony fringe of the exhausting palate with sharp and blunt dissection. Elevate the muscle off of the underlying nasal mucosa to raise a posteriorlybased oral myomucosal flap. Incise the best lateral incision from the bottom of the uvula to the best hamulus. Separate the clefted muscular tissues on the right from the sting of the exhausting palate to protect a rim of nasal mucosa to sew to . A, Elevation of superiorly primarily based pharyngeal flap with midline taste bud incision. C, Soft palate oral incision and posterior pharyngeal wall donor web site are closed primarily. D, Lateral view demonstrating place of the pharyngeal flap above the transverse plane of the palate and inset between the oral and nasal layers of the palate. The anteriorly based mostly nasal mucosal flap must be transposed to the proper and sewn to the nasal mucosa at the fringe of the hard palate on the proper with 4-0 absorbable sutures in a easy interrupted style. This flap is then sewn to the adjacent mucosal edges on each side; anteriorly to the nasal mucosal flap from the right, and posteriorly to the sting of the nasal incision along the posterior fringe of the taste bud. The right anterior-based myomucosal flap must be transposed to the left and sewn to the oral mucosa at the fringe of the hard palate. The tip of this flap must be close to the most inferior facet of the pharynx that can be seen with the mouthgag in place. A, Outlined incisions for sphincter pharyngoplasty involving posterior tonsillar pillar and inset incision in the posterior pharyngeal wall. C, Flaps are sutured together and inset with mucosal surfaces superficial and muscle-surface deep. D), Single nasopharyngeal port is thus created; donor site mucosal wounds are closed primarily. The flap should be elevated towards the cranium base, in a aircraft at or above the level of the exhausting palate. The dimension of the port may be personalized utilizing nasal trumpets as a guide, and suturing the divided palate more posteriorly to slim the port as needed. Sew the tip of the pharyngeal flap to the nasal layer on the most anterior facet of divided palate with 4-0 absorbable suture. Continue this inset laterally on both sides with mattress sutures till the flap is well secured to the palate. Reapproximate the oral mucosa of the midline palatal incision over the pharyngeal flap. On each side, the aperture of each port can be adjusted with the final few sutures. Ensure ultimate hemostasis, particularly in the most superior side of the bottom of the flap, which is a common space for bleeding. Place a nasal trumpet or 4-0 endotracheal tubes on both sides of the nostril and visualize passage into the pharynx through the ports. Once in an adequate place, these could be secured together with a transseptal sew; nasal trumpets may simply be taped to keep away from dislodgement. The aperture of the single velopharyngeal port may be controlled by the length of the flaps and the degree of overlap. Not stress-free the mouthgag regularly, leading to postoperative edema of the tongue. Arm restraints always for 2 weeks except when held and supervised for a brief time period 3. However, it might nonetheless be present, though more inconspicuous, in non-syndromic sufferers. In 2011, Robison and Otteson,1 reported a evaluation of 459 sufferers with cleft lip, cleft palate, or cleft lip and palate. In a separate paper, the same group reported a 28% constructive screening rate in non-syndromic sufferers evaluated in a craniofacial clinic. Cleft surgeons ought to routinely inquire about patient sleep habits and symptoms, even in patients with isolated cleft lip and or palate. Screening with a polysomnogram must be thought of in symptomatic sufferers, as airway interventions may be indicated. As at all times in cleft surgery, the objective is to obtain a reliable velopharyngeal port at the time of the initial palate surgical procedure. We have found that even with extensive clefts, the Furlow technique can be used efficiently in most patients. Incidence of optimistic screening for obstructive sleep apnea in patients with isolated cleft lip and/or palate. Screening for obstructive sleep apnea in kids handled at a significant craniofacial middle. Nasopharyngeal stenosis-Possible complication of each pharyngeal flap and sphincter pharyngoplasty. It is may end result from cicatricial scar in velopharyngeal port; surgical restore is necessary if it develops. Patients with orofacial clefting have increased charges of sleepdisordered breathing and obstructive sleep apnea compared to the final pediatric population. In the English language, the entire following consonant phonemes require the velopharyngeal valve to be open (nasal resonance), except: a. Management of velopharyngeal insufficiency: improvement of a protocol and modifications of sphincter pharyngoplasty. Patients usually current in infancy, years earlier than any surgical intervention is possible. This offers the microtia surgeon and the household time to develop a relationship and to contemplate acceptable surgical and nonsurgical options. When the time comes, profitable surgical reconstruction of the auricle requires an extensive information of the conventional anatomy of the auricle, meticulous consideration to detail, and atraumatic handling of tissues. Throughout the years of counseling, patients should be suggested regarding all choices for surgical repair, together with watchful ready, costochondral graft, exterior prosthesis, and use of an alloplastic implant. Worldwide, the most common methodology of repair remains the costochondral cartilage graft. Reference is made on the conclusion of the chapter to traditional articles masking different methods. An understanding of the thickness of the recipient skin pocket is crucial to avoid both extremes: (1) too thick with subsequent lack of ear definition; and (2) too thin with compromise of the pores and skin from ischemia. An applicable skin flap will end in glorious detail of the sculpted cartilaginous framework. Most auricular deformities will have been present from start, but it could be very important elicit any adjustments in improvement of the ear or history of trauma to the auricle.
Alli 60 mg cheap without a prescription
The pathophysiology of "progressive lacunar stroke" is incompletely understood weight loss pills sams club 60 mg alli purchase overnight delivery, and no treatment has been confirmed to stop or halt development weight loss 6 months after gastric bypass alli 60 mg buy low cost. Cavitation and lesion shrinkage are seen in more than 95% of deep symptomatic lacunar infarcts on follow-up imaging. Embolic infarcts are typically peripheral (cortical/subcortical) quite than the standard central and deep location of typical lacunae. Watershed or "border zone" infarcts grossly resemble lacunar infarcts on imaging research. However, "border zone" infarcts occur in particular locations-along the cortical and subcortical white matter watershed zones-whereas lacunae are extra randomly scattered lesions that primarily have an effect on the basal ganglia, thalami, and deep periventricular white matter. Anatomy of the Cerebral "Border Zones" Watershed zones are defined because the "border" or junction the place two or more major arterial territories meet. Etiology Two distinct hypotheses-hemodynamic compromise and microembolism-have been proposed because the etiology of hemispheric watershed infarcts. Terminal vascular distributions normally have decrease perfusion pressure than main arterial trunks. Maximal vulnerability to hypoperfusion is best where two distal arterial fields meet collectively. Hypotension with or with out extreme arterial stenosis or occlusion may find yourself in hemodynamic compromise. Anteriorly, they center within the posterior frontal Arterial Anatomy and Strokes lobe near the junction of the frontal sulcus with the precentral sulcus. Bilateral lesions are sometimes associated to international discount in perfusion strain, often an acute hypotensive occasion. Confluent infarcts are massive, cigar-shaped lesions that lie alongside or simply above the lateral ventricles. They resemble a line of beads extending from entrance to back in the deep white matter (8-63B). Nontraumatic Hemorrhage and Vascular Lesions 232 thalami, and pons and appear randomly scattered. Emboli are sometimes bilateral and multiterritorial but also can occur at vascular "border zones. Death or severe lifelong neurologic deficits, including motor impairment, cognitive deficiency, and developmental delay, are common. This section will emphasize the position of ischemia and hypoxia in perinatal brain injury and acknowledge that inflammatory elements. Focal ischemia refers to decreased or absent perfusion in a specific vascular territory. Global ischemia happens when total cerebral perfusion drops below the level required to preserve regular mind operate. From the center of the third trimester of being pregnant by way of the fortieth postconceptional week, the dorsal brainstem, thalami, basal ganglia, and perirolandic cortex exhibit excessive metabolic activity. Damage is mirrored in the interarterial (watershed) boundary or border zones and cerebral cortex (8-79A). In the 2nd trimester (gestational age of 14-26 weeks), ischemic harm results in liquefaction (8-80F); within the third trimester (27-40 weeks), ischemic injury leads to astrogliosis. Prolonged systemic hypoxemia results in cardiac hypoxia, which in turn diminishes cardiac output. Focal hemorrhage is demonstrated on the caudothalamic groove, which represents the situation of the best aggregation of germinal matrix tissue. Linear accumulations of intraventricular hemorrhage are demonstrated within the frontal horns. Arterial Anatomy and Strokes 235 (8-70A) Coronal post-mortem specimen exhibits expansile clot inside the left lateral ventricle. Note the bihemispheric hypointense halos, representing neurons migrating outward from the germinal matrix. During the period of early recovery (6-18 hours after insult), lactate and diffusivity abnormalities might transiently "normalize," solely to revert to abnormality after 24 hours. This just so occurs to complement the present mind cooling protocols that typically conclude on day four. Normally, blood vessels of the mind constrict when blood stress will increase and dilate when blood pressure decreases. In the time period new child, hypoxia and hypercarbia lead to the lack of cerebral vascular autoregulation. Physiologic monitoring is required, and sedation is often wanted to management movement. Cranial sonography is nicely suited to germinal matrix and intraventricular hemorrhage detection, and follow-up, is low cost, requires no sedation, is moveable to the bedside, and uses no ionizing radiation (8-67A). As an instance, maternal chorioamnionitis resulting in preterm delivery at 30 weeks (third trimester of pregnancy) with the subsequent discovery of periventricular white matter damage likely represents a perinatal injury, not essentially a neonatal harm. This nuance of understanding has practical implications for our neuroimaging reviews due to attainable obstetrical and fetal maternal drugs authorized consequences. The perinatal time-frame is defined because the interval beginning at 20-28 weeks of gestation prior to delivery and lengthening 14 weeks after start. Note the absence of expected T1 shortening (myelination) inside the posterior limbs of inside capsule. Ca++, manganese, and lipids within injured tissue could contribute to T1 shortening. The spectrum of brain injury within the preterm and term neonate is surprisingly broad with distinctive qualities and factors of overlap. The full appraisal of harm is determined by the timing of imaging and the imaging modality chosen. Preterm newborns are born before 37 weeks of gestation and usually weigh less than 1,500 g. For those that survive prematurity, 90% will manifest neurologic deficits, together with cerebral palsy and cognitive, behavioral, and a focus deficit disorders. The prevalence and severity of neurologic sequelae increase with the extremes of prematurity. Lateral ventricles are compressed, distinguished regular torcula due to surrounding edema. Diffusion restriction is inside the corticospinal tracts and superior cerebellar vermis. T2 prolongation is commonly seen in affected areas within the first few days after damage, and T1 shortening may be detected after three to 4 days. Given the diffuse cerebral harm (neurons and axons) past simply white matter, a more correct encompassing but less generally used description is encephalopathy of prematurity.
Order 60 mg alli with visa
A comparison of resource cost for head and neck reconstruction with free and pectoralis major flaps rapid 60 weight loss pills alli 60 mg generic free shipping. Comparison of the rectus abdomens free flap with the pectoralis major myocutaneous flap for reconstructions within the head and neck weight loss pills lipo 6 buy alli 60 mg lowest price. Which of the following is a relative contraindication to utilizing a pectoralis major flap Pharyngeal reconstruction in the patients with vessel-depleted multiply operated necks d. A 78-year-old moribund patient underwent a composite resection for treatment of regionally superior squamous cell carcinoma of the oral cavity; previous palliative radiation had failed. The entire process was carried out on the idea of a weight-based heparin nomogram and aspirin in view of lately positioned cardiac stents and symptomatic cerebrovascular disease. General "nonsurgical" oozing is noted in the lateral facet of probably the most cephalad a half of the dissection pocket. A 69-year-old edentulous man with squamous cell carcinoma of the oral cavity invading left mandibular parasymphysis (T4 N0) underwent composite resection with bilateral neck dissection and reconstruction with an osteocutaneous free fibula flap. On postoperative day 1, the patient was taken back to the working room for venous congestion and underwent venous thrombectomy. Despite postoperative anticoagulation, necrosis of the intraoral skin paddle developed and salivary leak into freshly dissected neck ensued. The affected person was once more returned to the operating room the place the free fibula was discovered to be utterly necrotic. Placement of radial forearm fasciocutaneous free flap over the existent mandibular plate b. Placement of pectoralis major musculocutaneous flap to cowl the existent reconstruction plate. Removal of the plate and pectoralis main musculocutaneous flap (mandibular swing) 1190. Since the introduction of this technique within the 1960s, the potential of reliably transposing massive volumes of vascularized tissue for reconstruction has revolutionized our capacity to resect illness and safely reconstruct defects within the head and neck. Although important focus was positioned on the role of free flaps for reconstruction in the course of the Eighties and Nineties, current years have introduced a rebirth of curiosity and enthusiasm for the usage of regional flaps. An perfect reconstruction provides a patient with the best outcome (in each function and form) with the bottom donor-site and total morbidity. Flaps from the cervicofacial area embrace both randompattern vascular flaps (cervicofacial flaps) and axial vascular sample flaps (cervicopectoral, supraclavicular, deltopectoral, and submental flaps). A comprehensive understanding of regional anatomy allows for the use of a number of regional flaps to reconstruct defects within the head and neck. Planning for the vascular pedicle and its final geometry are of key importance for flap viability and success in reconstruction. Prior remedy within the head and neck region 1) Prior head or neck surgical procedure could affect the viability of regional reconstructive options. Medical diseases that will affect flap viability and reconstructive outcomes 1) Diabetes, particularly if poorly controlled, can have an effect on therapeutic outcomes and flap viability. Family medical history 1) Coagulopathies can promote postoperative bleeding or coagulation and thus flap viability. Medications 1) Consideration of risks/benefits to discontinuing any drugs that might improve the danger of bleeding. The face should be rigorously evaluated for any scars or proof of prior surgical intervention, as this might disrupt blood move for a cervicofacial advancement flap. The dimension of the defect should be measured to make positive that the planned flap is large sufficient to cover the defect. The neck must be rigorously evaluated for any scars or evidence of prior surgical intervention which will have an effect on blood move. In planning a submental island flap, the amount of submental skin redundancy have to be measured by way of the "pinch test," with the patient in mild neck extension to guarantee enough flap quantity whereas sparing enough tissue for closure of the primary donor website without proscribing head elevation. A preoperative Doppler examination ination is required for the supraclavicular artery flap to identify and hint the vascular pedicle from the supraclavicular fossa over the clavicle and onto the deltoid area of the shoulder. The extent and complexity of the defect requiring reconstruction should be decided. It might help in surgical planning to establish that the vessels of the flap pedicle are intact. The accessory nerve is at risk during elevation and rotation of the sternocleidomastoid muscle flap. It ought to be identified, dissected free of the muscle, and preserved throughout flap elevation/rotation. The cervicofacial flap is a fasciocutaneous flap primarily based off of a random blood supply; it encompasses tissue from the facial and cervical regions. This is essentially the most commonly used anesthetic method as a end result of the flap is usually harvested concurrently with tumor resection. General anesthesia is useful in procedures that require dissection of the vascular pedicle, since this requires meticulous care. Use of a paralytic is on the discretion of the surgeon relying on the nerves in danger. Unmatched in its ease of harvest, ability to resurface massive defects, good shade match, and esthetic result with minimal donor-site morbidity b. Placement of a shoulder roll or extension of the neck away from the side of operation may be useful throughout early flap elevation. At the end of the surgery, if the closure is underneath tension, contemplate eradicating all rolls and rotating the patient back to neutral position to reduce tension and aid in primary closure. The primary limitation of the flap is that, due to its random blood supply, it requires a large base for maximal vessel recruitment and vascularity could additionally be compromised at its distal edges. Patients with prior radiation remedy, surgery, or significant peripheral vascular illness are extra weak to ischemic lack of the flap. Advancement and rotation of the flap can result in a temporary standing-cone deformity. Their use is dependent upon the defect to be reconstructed and the associated danger components. Standard head and neck set Bipolar cautery Sterile Doppler Spy fluorescent angiography-allows for the prediction of flap viability after harvesting Operative Risks 1. Suction drains should be positioned every time possible owing to the significant lifeless area created during flap elevation and threat of hematoma formation. Cervicofacial flap design (A to D): Patient with a defect within the anterior right cheek after resection of a pores and skin most cancers. A, the posterior limb is carried horizontally to the preauricular region and then continued around the lobule within the postauricular tissue to increase the potential arc of rotation. Horizontal skin creases in the lower neck are marked and the extent of horizontal transition depends on the arc of rotation needed.
Alli 60 mg cheap with visa
In addition to together with the pericranium and immediately superficial free areolar tissue weight loss news alli 60 mg order with mastercard, this flap contains the galea weight loss pills kenya alli 60 mg purchase without prescription, thereby providing the reconstructive surgeon with a thicker pedicled flap. History of Present Illness Patients who current to the cranium base surgeon often require a multidisciplinary approach to guarantee correct analysis and analysis for optimum therapy. A detailed description of this important portion of the analysis is outdoors the scope of this chapter, but ought to concentrate on figuring out clinical options that afford insight into the scientific development, involved primary and adjoining constructions, and the potential for regional or distant disease. This data should information further investigations and body patient counseling. Medical Comorbidities 1) Diabetes mellitus, hypercortisolism, poor dietary status, and cigarette smoking are risk elements for delayed wound healing and should be taken into account by the surgical group. Medications 1) All efforts ought to be made to maintain antiplatelet and anticoagulants previous to surgical intervention to minimize the chance of excessive bleeding or the development of a hematoma in the donor website or surgical web site. The pericranium contains the calvarial periosteum and related areolar tissue lying deep to the galea. Physical Examination A comprehensive bodily examination is of upmost significance when evaluating patients for skull base surgical procedure. The bodily examination ought to think about findings that point out the degree of tumor extension together with local mass impact and cranial nerve neuropathies. Suspected harm to the vascular provide or prior utilization primarily eliminates its use in reconstruction of the skull base. Evaluation of the hair and hairline also wants to be famous, as a result of it will assist the reconstructive surgeon plan the incisions for flap entry. Additionally, the facial skeleton and position of the calvarial convexity should be noted, as a result of an incision placed anterior to or posterior to the convexity might make complete elevation of the flap challenging when using an endoscopic-assisted method. Bilateral sinonasal endoscopy offers the reconstructive surgeon with crucial data relating to the placement of the tumor and helps to determine the supply of intranasal vascularized flap options. Defects localized to the posterior fossa/clivus; the defect generally lies on the distal-most side of an prolonged flap with the risk of poor or insufficient coverage of the defect. These research are important in allowing the skull base group to assess the burden of illness, surrounding important neurovascular buildings, candidacy for resection, and the projected surgical defect. Such studies can also present clues to the availability of intranasal vascularized flaps that will not be apparent on sinonasal endoscopy. Imaging studies for staging ought to be sought in patients with malignant tumors to ensure applicable treatment objectives and therapy planning. Paralysis might or is most likely not used and is dictated by the necessity for neurophysiological monitoring through the resection portion of the operation. Positioning At the discretion of the surgeon, the affected person could additionally be placed in a supine position or in a modified "seaside chair" position, with the top of the mattress elevated and feet lowered. Occasionally, a light degree of reverse Trendelenburg can also be used to optimize positioning and help in visualization. Using a 3-cm correction issue accounting for flap transposition via the nasionectomy and retraction, the following flap length estimates had been needed to reach the following defects: eleven. Endoscopic monopolar and bipolar cautery, endoscopic clip appliers with an array of hemostatic clips, hemostatic agents, and an array of pledgets. Line-of-sight image steerage is usually favored in open procedures or these utilizing pin immobilization. The alternative between line-of-sight and electromagnetic image steerage is that of the working surgeon, as a outcome of each modalities provide comparable info. A commonplace coronal incision is made beginning in the preauricular area and traversing to the contralateral preauricular region. Once the incision is made, the plane between the subgaleal fascia and overlying galea is identified and the coronal flap is elevated anteriorly in this aircraft. Given the lateral extensions of the incision, the frontal branches of the facial nerve are recognized and are elevated with the galea. Once the tumor extirpation or different pathology has been addressed, consideration is turned to the reconstruction portion of the process. Depending on the extent of dural involvement and dissection, some type of synthetic dural substitute is often used for preliminary dural restore and placed in an underlay trend to cover the defect. The scalp incision is planned as an ipsilateral hemicoronal incision, which is positioned in a trichophytic style on the hairline near the midline and continued to the temporal hair tuft in standard hemicoronal style. The true skin incision is generally solely approximately 3 to four cm in length and is often limited to probably the most superior aspect of the hemicoronal incision, however could also be lengthened in either path as essential for flap publicity. Prior to the incision, a Doppler ultrasound probe can be used to identify the supraorbital and supratrochlear vessels, at which level a 3-cm-wide flap pedicle is outlined with the pedicle marked within the midline at the supraorbital rim. Subgaleal dissection may be aided with the use of 0- and 45-degree rigid endoscopes, which provide high-definition and magnified photographs of the dissection. Once an enough posterior size is achieved, typically roughly 15 cm posterior from the brow, a horizontal incision is made right down to the pericranium on the posterior aspect of the flap with the use of extended needle tip cautery under direct endoscopic visualization. The pericranium is the calvarial periosteum extending concerning the cranial convexity within the midline with the lateral boundaries delineated by the superior-most facet of the temporalis muscles and their overlying fascia. Immediately superficial to the pericranium lies unfastened areolar tissue followed by the galea. At the discretion of the reconstructive surgeon, both of these layers can be included into the flap to present a thicker flap depending upon the reconstructive needs. The supraorbital and supratrochlear arteries present axial vascular provide to the flap. The place of the vascular provide could be recognized utilizing a Doppler probe or the supraorbital notch may be palpated and a flap pedicle width of 3 cm (1. The nasion is essentially the most depressed portion of the nostril on profile view and is generally on the intersection of the frontal process of the nasal bones and nasal means of the frontal bones. A surgical window created at this web site, termed a nasionectomy, affords intranasal access simply anterior to the anterior facet of the frontal sinus outflow tract. Endoscopic skull base coaching is highly beneficial due to the particular necessities of this procedure. The prime neurovascular constructions at risk are the supraorbital and supratrochlear vessels and the supraorbital nerve. With a radical understanding of the trajectory of these structures, they might be successfully prevented and the sensory and motor functions of the scalp could be preserved. A, Progressive elevation of the scalp inside the subgaleal plane permitting for the isolation of the underlying pericranium. B and C, Following isolation of the pericranium, monopolar cautery is used to carry out circumferential incisions concerning the pericranium with care taken to preserve a 3-cm-wide pedicle at the proximal facet of the flap within the region of the superior orbital rim (arrow). Attention is then turned to the glabella, where an approximately 1-cm, horizontal skin incision is made in a natural pores and skin crease and carried right down to the periosteum at the stage of the nasion. Direct visualization of the ostectomy using the endoscope allows for secure drilling and minimizes potential harm to surrounding buildings. The edges of the flap are typically bolstered with a bioresorbable nasal dressing that assists in minimizing the formation of adhesions and supplies mechanical compression. A layer of an absorbable hemostatic agent is then applied, adopted by intranasal, expandable packing sponges, which help to support the reconstruction. The scalp and nasion incisions are then closed primarily in a multilayered fashion. Additionally, it may be very important be aware that some size shall be misplaced with rotation and contracture of the flap.
Alli 60 mg buy on line
One blade of the scissors is inserted simply contained in the lateral canthal angle; one is positioned on the skin weight loss pills online alli 60 mg sale. The vary of intraocular pressures was from 30s to 80s after intraorbital injection weight loss pills las vegas purchase 60 mg alli fast delivery. Seven orbits achieved a ultimate strain of less than 20 mm Hg with a lateral canthotomy and inferior cantholysis alone. The two orbits required an additional superior cantholysis to obtain a whole decompression, as described by the authors as a final intraocular pressure of less than 10 mm Hg. Lateral canthotomy is a quick however critical procedure for every otolaryngologist to be conversant in. Its use in emergency situations (increasing proptosis of any kind) and its place as the first step of different surgical procedures require cautious rote memorization of the steps in this procedure and follow on a cadaver if attainable. The medical administration of retrobulbar haemorrhage complicating facial fractures: a case report. Patients at risk, but have but to develop orbital compartment syndrome, may be conservatively managed with serial examinations, however these ought to be limited to instances with shut collaboration with ophthalmology. Which of the following signs should raise the suspicion of orbital compartment syndrome developing Monocular diplopia (double vision solely current with the unaffected eye is closed) d. Somecancersarisingin the skin may even require complete or subtotal removing of the orbitalcontents. Most fungal infections of the orbit unfold from adjoining sinuses, and two main varieties occur. Patient with malignant melanoma destroying the globe, adnexa, and orbital contents. Itisinappropriate in any tumors affecting the skin, conjunctiva, or lacrimal gland. Lid-sparing exenteration offers a superb color match to surrounding skin and heals comparatively rapidly. B, Computed tomography scan demonstrating invasion of the orbit and destruction of the bony orbital wall. Patient 1 year after left orbital exenteration for adenoid cystic carcinoma arising in left maxilla, reconstructed with an anterolateral thigh free flap. The latter is tightened to a delicate cease and tightened sequentially over a period of several minutes to assist with hemostasis. The area is coated lightlywithantibioticointment,andthepatientandfamily are instructed to repeat the appliance of ointment twice daily. Common Errors in Technique � I t is posteromedially that an iatrogenic cerebrospinal fluid leak could also be created, either by direct trauma or by theuseofmonopolarcautery,whichmaytravelthrough emissary foramina or dehiscences. The former could also be drained by making a small incision within the graft, gently evacuating the hematoma, after which changing the pressuredressingfor2to5days. Alternative Management Plan � When tumor entails each orbital apices, different palliative optionsshouldbesought. Despite multiple makes an attempt to clarify and higher define its oncologic indications,controversyabounds. Nonetheless,aspointedoutin this chapter, the current literature supports some essential conclusions. Its association with poorer outcomes is most likely going the outcomes of tumors that are more aggressive. Imaging evidence of frank invasion of the medial rectus muscle in the setting of an ethmoid tumor 2. The most secure approach to establish hemostasis of the apical stump in an orbital exenteration is through the use of monopolar cautery to divide the optic nerve on the annulus of Zinn. Rehabilitationoforbital cavity after whole orbital exenteration using oculofacial prostheses anchored by osseointegrated dental implants posed as a one-step surgical procedure. Management of the orbital contents in radical surgery for squamous cell carcinoma of the maxillary sinus. Rhinoplasty includes functional, cosmetic, and reconstructive surgery to tackle the function and look of the nose. Functionally, the airway begins on the nostril, and issues corresponding to static or dynamic collapse (collapse on inspiration) might present at the degree of the external or inner nasal valve. The anterior projection of the nostril on the face makes nasal reconstruction an artwork that combines the useful and aesthetic aspects of rhinoplasty. True mastery of rhinoplasty, with all its aesthetic and functional nuances, requires an extended studying curve and the devoted focus of a growing surgeon. Physical Examination � A full examination of the head and neck ought to be carried out, with explicit consideration to the exterior nasal anatomy. A practical affected person with smart expectations is the inspiration for a constructive end result. Managing affected person expectations is crucial to the preoperative and postoperative course. A full panel of rhinoplasty pictures should be taken, together with frontal, indirect, basal, lateral, and lateral smiling. Inthecase of open rhinoplasty, this contains the transcolumellar incision, marginal incisions, and within the subcutaneous plane all through the skin-soft tissue envelope and osteotomy websites. Hemostasis could be achieved by bipolar cautery or stress however is normally not needed until dissection was carried out laterally into branches of the angular artery anastomosis. The marginal incision is made just caudal to the lateral crus and dissection adopted on the superficial surface. This strategy can be used for the septoplasty and is especially helpful in instances of severe deviations of the caudal septum causing nasal vestibular stenosis. We will now divide the nasal skeleton into thirds from superior to inferior and outline manipulations that may affect the looks and function of the nose. Incasesofadeficientprojection of bony pyramid, grafting may be carried out with autologous cartilage with or with out muscle fascia or perichondrium to increase the nasion. Unlessthenasalbonesare medialized with lateral osteotomies, the affected person may be left with an open roof deformity. The transcolumellar incision is accomplished sharply with the tissue scissors, making sure to keep superficial to the medial crura. The percutaneous osteotomy method has advantages when dealing with severe upper third nasal deformities where extensive dorsal osteotomy work is necessary to mobilize old fractures. M iddlethird � the center third of the nostril consists primarily of the upper lateral cartilages and their attachment to the septum. This maneuver ought to be done with care, as overresection of the dorsal septum can result in practical and cosmeticissues. Theselong,flatgrafts typically made out of septal or auricular cartilage present dorsal support to the center vault and stop or deal with center vault collapse. A, the pores and skin envelope is retracted whereas sharp dissection is used to elevate the pores and skin envelope from the tip cartilages. B, Inferior retraction of the nasal tip cartilages aids in dissection towards the nasion.
60 mg alli purchase fast delivery
Neuronal and Mixed Neuronal-Glial Tumors Neuroepithelial tumors with ganglion-like cells weight loss hypnosis buy 60 mg alli otc, differentiated neurocytes weight loss pills australia alli 60 mg buy generic online, or poorly differentiated neuroblastic cells are characteristic of this heterogeneous group. Other tumors on this class are desmoplastic infantile astrocytoma and ganglioglioma, neurocytoma, papillary glioneuronal tumor, rosette-forming glioneuronal tumor, and cerebellar liponeurocytoma. Two alternative ways of taking a glance at medulloblastoma-as genetically outlined or histologically defined-are included. Some of the genetically outlined and recognized histologic variants are related to dramatically completely different prognoses and therapeutic implications. They come up from leptomeningeal melanocytes and could be diffuse or circumscribed, benign or malignant. Tumors of Cranial (and Spinal) Nerves Schwannoma Schwannomas are benign encapsulated nerve sheath tumors that consist of well-differentiated Schwann cells. Although their incidence has increased slightly over the past twenty years, lymphomas are still significantly much less common than glioblastoma and different malignant astrocytomas. The much less common papillary kind is normally solid and found virtually completely in adults. Miscellaneous Sellar Region Tumors Granular cell tumor of the neurohypophysis, additionally called choristoma, is a uncommon tumor of adults that normally arises from the infundibulum. Pituicytomas are glial neoplasms of adults that additionally normally arise throughout the infundibulum. Spindle cell oncocytoma of the adenohypophysis is an oncocytic nonendocrine neoplasm. The diagnosis is normally histologic, as differentiating these tumors from each other and from different grownup tumors such as macroadenoma can be problematic. They can be mature, immature, or happen as teratomas with malignant transformation. Sellar Region Tumors the sellar region is doubtless considered one of the most anatomically complicated areas in the brain. The sellar area contains many structures besides the craniopharyngeal duct and infundibular stalk that give rise to masses seen on imaging studies. Intracranial Cysts Cysts are widespread findings on neuroimaging studies and, for purposes of dialogue, included on this part of the text. There are 4 key anatomy-based inquiries to pose when contemplating the imaging prognosis of an intracranial cyst. Although many cysts can be present in a number of places, every kind has its own "most popular". The three main anatomic sublocations are the extraaxial areas (including the scalp and skull), the brain parenchyma, and the cerebral ventricles. Pituitary Adenoma Pituitary adenomas account for the majority of sellar/suprasellar masses in adults and the third commonest overall intracranial neoplasm in this age group. Pituitary adenomas are categorized by size as microadenomas (10 mm) and macroadenomas (11 mm). It shows a definite bimodal Extraaxial Cysts that is the second largest group of nonneoplastic cysts. The chapter on nonneoplastic cysts considers these first, beginning from the scalp and cranium and proceeding inward to Introduction to Neoplasms, Cysts, and Tumor-Like Lesions 507 (16-11) A gelatinous cyst at the foramen of Monro splays the fornices and enlarges the lateral ventricles, whereas the third ventricle is normal. The unusual but necessary "neoplasmassociated cysts" which may be typically seen round extraaxial tumors such as macroadenoma, meningioma, and vestibular schwannoma are most likely a form of arachnoid cyst. Neuroglial cysts-parenchymal cysts lined by nonneoplastic gliotic brain-are comparatively uncommon. Intraventricular Cysts Intraventricular cysts are much less common than cysts in the brain parenchyma. The most common intraventricular cysts are choroid plexus cysts, that are virtually all the time incidental findings on imaging studies. Chapter 17 509 Astrocytomas Gliomas account for barely lower than one-third of all intracranial neoplasms and over 80% of the first malignant ones. Astrocytomas are the single largest group of neoplasms that come up inside the mind itself. Astrocytomas type a surprisingly diverse group of neoplasms with many different histologic varieties and subtypes. These fascinating tumors differ extensively in preferential location, peak age, clinical manifestations, morphologic features, biologic behavior, and prognosis. For purposes of our dialogue, astrocytomas are organized into two common classes: a relatively "localized," comparatively more benign-behaving group and a "diffusely infiltrating," more biologically aggressive group. This distinction is considerably arbitrary and imperfect, as some "circumscribed" astrocytomas often turn out to be extra aggressive and infiltrate adjacent constructions regardless of their low-grade histology. Origin of Astrocytomas Astrocytomas had been initially named for his or her putative origin from the stellate-shaped cells-"astrocytes"-that are the dominant part of the neuropil (vastly outnumbering neurons). It was as quickly as assumed that astrocytes might bear both hyperplasia (nonneoplastic "reactive astrocytosis") and neoplastic transformation. Instead, they most likely develop from distinct populations of precursor "glioma-initiating" cells that possess stem cell properties. Characteristics of most cancers stem cells embrace (1) capability for self-renewal, (2) differentiation potential, (3) excessive tumorigenicity, (4) drug resistance, and (5) radioresistance. Subsequent mutations lead both to astrocytomas (blue) or oligodendrogliomas (green). We focus on astrocytomas in this chapter; oligodendrogliomas are grouped with other nonastrocytic glial neoplasms and mentioned in Chapter 18. The vast majority of astrocytomas develop extra rapidly, diffusely infiltrate adjoining tissues, and display an inherent propensity to undergo malignant degeneration. Classification In the past, classification was based mostly virtually solely on histologic phenotype. Now, once the preliminary diagnosis of a diffuse glioma is established by long-established histologic criteria, gliomas (whether astrocytic or not) are grouped into subtypes based on the presence or absence of particular genetic parameters. Astrocytomas 511 (17-3) Childhood pilocytic astrocytomas occur within the cerebellum and hypothalamus/optic nerves. Age and Location in Astrocytomas Diffuse astrocytomas in childhood look microscopically like their adult counterparts but exhibit distinctly completely different biologic behaviors. One of the most hanging is the effect of age on each astrocytoma subtype and most popular location. Some astrocytomas (such as pilocytic astrocytoma) happen nearly solely in children, whereas others. There can be a very strong anatomic choice with some tumors in sure age groups occurring regularly in some locations and very not often in others. Approximately 75% of all major brain tumors in youngsters happen in the posterior fossa, whereas the reverse is the case in adults. Astrocytomas in children are sometimes localized tumors that happen mostly in the posterior fossa or optic pathway.
Alli 60 mg purchase on line
Whereas recurrence rates are approximately 3% for branchial anomalies with no preceding surgeries or infections weight loss pills europe 60 mg alli discount free shipping, this rate rises to roughly 20% if there was a earlier unsuccessful surgical procedure weight loss 77080 60 mg alli order free shipping. The recurrence price following the excision of a sinus or fistula tract is roughly twice that following the excision of an isolated cyst. The identification and monitoring of the recurrent laryngeal nerve when anomalies of the third or fourth branchial pouch are being excised can reduce this risk. Prenatal imaging of the fetal branchial cleft cyst by three-dimensional ultrasound. Editorial Comment Branchial cysts and sinuses are the second most common congenital neck plenty. Knowledge of the embryology of the branchial equipment is essential for making an correct analysis, understanding the anatomy of those lesions, and excising them successfully. The surgical administration of branchial cysts and sinuses has remained basically the identical through the years apart from the addition of endoscopic management of third and fourth branchial anomalies. While excising a congenital mass within the neck, a sinus tract is famous that runs between the inner and external carotid arteries and travels both superior and lateral to the glossopharyngeal and hypoglossal nerves. The posterior displacement of the bottom of the tongue functionally obstructs the airway, causing apnea, stridor, problem with feeding, and retarded growth. The scientific severity of this obstruction can vary from subtle hypopneas, which can be famous solely on a sleep research, to dramatic life-threatening respiratory compromise that requires emergent airway intervention. Initial nonsurgical management of tongue-base-related obstruction includes susceptible positioning and placement of a nasopharyngeal airway. However, these measures may complicate already tenuous feedings and may enhance the chance for sudden infant demise in an unmanaged setting. Tongue-baserelated obstruction has historically been surgically addressed by tracheostomy to bypass the obstruction. However, this carries a low, however real threat of mortality from mucous plugging and different airway compromise. However, high charges of dehiscence, feeding difficulties, and recurrence of obstruction have been reported. Since then, a quantity of research have demonstrated goal enchancment in both feeding and airway measures, together with reduced apnea-hypopnea index, reduction of hypoxemia and hypercapnia, and elevated rates of per oral nutrition. Careful dealing with of soppy tissue throughout entry to the toddler mandible is important in avoiding iatrogenic nerve damage. It is necessary to take a careful birth historical past, including prenatal analysis by ultrasound or eliciting any problems with pregnancy or supply. Birth history must also embrace any preliminary airway misery and want for airway intervention, together with inclined positioning, nasopharyngeal airway, or intubation. If the toddler is feeding orally, the dad and mom ought to be requested a few typical feeding, together with the quantity of feeds, the period of each feeding, and any issues for aspiration. Decreased volumes or increased time for feeding may indicate an issue with the coordination of respiratory and swallowing. A cautious evaluate of the start historical past, initial hospitalization, earlier evaluations, and interventions to address airway and feeding issues must be undertaken. Other medical issues, congenital anomalies, or recognized genetic analysis should be reviewed. Observation of the toddler respiratory at rest may reveal signs of stridor or stertor, nasal flaring, subcostal or suprasternal retractions. Flexible nasolaryngoscopy may be carried out on the bedside to assess the patency of the choanae bilaterally, laryngomalacia, and degree of tongue base collapse. Measurement of the discrepancy between the central portion of the maxillary alveolar course of and the mandibular alveolar process can be made simply by placing the picket end of a cotton-tipped applicator alongside the anterior fringe of the mandibular gingiva in the midline. The maxillary gingiva will then contact the picket applicator, creating a natural marking on the wood due to saliva. However, if that is unclear, then markings may be made by pinching with two fingers or by a marking pen. The distance from the tip of the applicator to the marking indicates the diploma of maxillary overjet. Care have to be taken to keep away from posterior strain on the mandible, which can cause retropositioning of the mandibular condyle out of the immature glenoid fossa, thereby accentuating the maxillary-mandibular discrepancy. Orbital morphology may help distinguish Stickler syndrome, 22q deletion syndrome, or Treacher-Collins/ Nager syndrome. Malar projection should be famous as ought to any anomalies of the ear, together with microtia, pre-auricular remnants, or branchial arch anomalies. Patients with significant maxillary hypoplasia could show minimal maxilla-mandibular discrepancy despite having severe micrognathia. Patients with tongue base collapse because of microretrognathia who reveal indicators of airway obstruction by increased work of respiration, desaturation, hypoxemia, hypercapnia, or obstructive sleep apnea on polysomnogram. In sufferers with blended apnea, it has been demonstrated that many of the central apneic occasions noted on sleep research improve after decision of the obstructive element. However, patients with severe central sleep apnea or central hypoventilation would require positive stress air flow and should be thought of for a tracheostomy. Computed tomography scan of the mandible with 3D reconstruction exhibiting key landmarks in white and planned "inverted-L" osteotomy in blue. This osteotomy place avoids the most posterior creating tooth bud, which is usually positioned in the place marked "Ramus-Body Junction. In our middle, we carry out laryngoscopy and bronchoscopy with an endotracheal tube loaded on a Hopkins-rod telescope. The endotracheal tube is handed over the Hopkins-rod telescope in a Seldinger method when the scope is simply above the carina. Often a suture in the tongue is employed to distract the tongue anteriorly during laryngoscopy. Experience with the surgical care of neonatal patients Positioning Supine: the patient is positioned on a shoulder roll such that the neck is prolonged and capable of be turned from side to aspect. Damage to second/third molar tooth follicles Perioperative Antibiotic Prophylaxis Weight-based cephazolin is administered inside half-hour previous to the pores and skin incision. Prophylactic antibiotics are continued until the extension rods are eliminated when activation is complete. A typical preoperative view showing marked microretrognathia (A) and a postoperative view of the identical patient just previous to removing of distractor hardware (B). To keep away from injury to the facial nerve or its branches, make a skin only incision at the desired exit site and then bluntly dissect between the angle of the mandible and the exit web site to create a tunnel. Disparate distraction vectors: avoid these by ensuring that the distractor barrels are positioned parallel to the mandibular boarder. An additional analgesic (acetaminophen) dose is given half-hour prior to the turns of the activation rods.
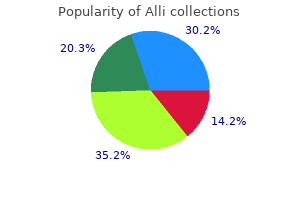
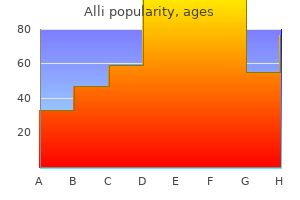
Real Experiences: Customer Reviews on Alli
Ayitos, 37 years: If cortisol levels stay high, then it is a signal of Cushing syndrome as a outcome of an adrenal gland tumor, which is producing cortisol.
Lars, 50 years: The treating physician can confirm this with sleep video-sonograms readily recorded by caretakers given the widespread availability of cellular phone video cameras.
Rocko, 41 years: It is skinny for orbital grafting and powerful for recreation of the facial buttresses.
Rhobar, 25 years: Age at analysis is a crucial prognostic characteristic, unbiased of tumor location.
Aila, 51 years: Radiographic dimension, location, diploma of listening to loss, and involvement of adjoining buildings will dictate probably the most advantageous surgical approach.
Mamuk, 24 years: Glands improve or decrease hormone production based mostly on the level of hormones in the blood.
Bernado, 54 years: Use caution to not puncture the globe with a curved suture needle when suturing the tarsal strip.
Vak, 48 years: Given the anterior angulation of the petrous pyramid, it must be designed such that 2/3 of the craniotomy opening is anterior to the exterior auditory canal.
10 of 10 - Review by R. Corwyn
Votes: 64 votes
Total customer reviews: 64
