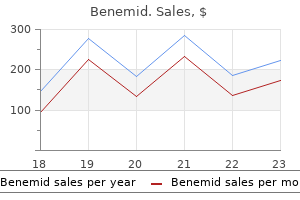
Benemid dosages: 500 mg
Benemid packs: 60 pills, 90 pills

Buy benemid 500 mg cheap
Lahey and Warren4 also famous that in 1886 Maydl reported excising a carotid physique tumor with division of the widespread, internal, and exterior carotid arteries pain medication for uti infection cheap 500mg benemid fast delivery. These early attempts included ligation and resection of the carotid artery bifurcation but no makes an attempt at reconstruction joint and pain treatment center thousand oaks quality 500 mg benemid. The tumor recurred as its unique site inside a year and required re-excision, as reported by Keen and Funke5 and Paltauf. By the Nineteen Sixties and Seventies, several hundred circumstances of carotid physique tumors had been reported, but the complication charges related Histology Carotid body tumors include epithelioid cells grouped into cords or clusters, also recognized as Zellballen. Several reviews have detailed the chromaffin-positive nature of the secretory granules, indicating that the carotid physique and tumors of it might be able to secreting catecholamines similar to norepinephrine and dopamine. Clinical Presentation the commonest manifestation of carotid physique tumors is a palpable neck mass in the high cervical area. Less frequent preliminary presentations include cranial nerve deficits similar to laryngeal dysfunction (hoarseness), problem swallowing, and unilateral tongue atrophy or weak point. The ascending pharyngeal artery typically provides many of the vascular provide, and the superior thyroid artery almost always provides a minority contribution. If angiography is planned, a concomitant session to embolize the tumor can be coordinated. Studies have proven that preoperative embolization considerably reduces blood loss during resection of a carotid body tumor. Clinicians should be conscious of the potential comorbidity of a pheochromocytoma and that some carotid physique tumors secrete catecholamines. In such patients, -adrenergic blockade have to be induced pharmacologically 2 weeks before surgical procedure. Once the predominance of carotid physique tumors in girls remains to be obvious, at a ratio of two: 1. An autosomal dominant expression of bilateral tumors, nevertheless, happens in 32% of patients with a familial prevalence. Gardner and coworkers25 reviewed 11 patients with carotid physique tumors, three of whom had other head and neck paragangliomas. Seminal genetic research have indicated an increased expression of the oncogenes c-myc, bcl-2, and c-jun in most carotid body tumor specimens studied. Characteristics of Tumor Growth In an effort to assess the preoperative risks of tumor resection, Shamblin and associates36 revised a classification scheme for carotid physique tumors. In this difficult group, the superior laryngeal and hypoglossal nerves might traverse the tumor. They are problematic only of their local invasion of vascular and nervous buildings and, occasionally, the oropharynx. Distant metastases have been reported in lymph nodes, bone, lung, liver, pancreas, thyroid, kidney, mind, and breast. Surgical Treatment Preoperative planning is crucial to reduce morbidity in sufferers with carotid body tumors. As talked about, an intensive medical analysis is important, notably to rule out endocrine abnormalities. Preoperative embolization helps reduce blood loss throughout resection, however diagnostic cerebral angiography is equally necessary for assessing collateral blood move. In such circumstances, surgeons might anticipate intraoperative shunting to take care of enough cerebral blood circulate. For instance, a small group I tumor could also be accessed via a transverse incision alongside a cervical pores and skin crease, giving the best cosmetic result. Here, an oblique incision along the medial border of the sternocleidomastoid muscle is indicated. As in a normal exposure for carotid endarterectomy, the common facial vein is ligated and minimize to mobilize the jugular vein laterally. Frequently, the hypoglossal nerve may be displaced superiorly and posteriorly by the tumor8; consequently, care should be exerted throughout dissection of the superior aspect of the tumor to keep away from damaging this nerve. Tumor invasion into the carotid arterial wall requires short-term occlusion with, or without shunting, to dissect the tumor and, if necessary, high patch the arterial wall defect with a graft. Interestingly, first bite pain occurred in 10 of 25 patients assessed postoperatively. Radiosurgery could also be helpful for a metastasis or intracranial extension, however, no significant sequence of this relatively rare pathology has been reported so far. Collagen and ground substance accumulate in the inner media in the milder type of the disease, separating within the disorganized smooth muscle cells. In the severe kind, the media is profoundly disorganized, with fibroblasts and collagen replacing the smooth muscle. In these larger tumors, the risk of prolonged carotid occlusion is more doubtless. In the excessive cervical exposure, the indirect incision is sustained in a curvilinear trend anterior to the tragus as much as the basis of the zygoma. Mobilization of the parotid gland is commonly essential in these giant carotid physique tumors, so the temporoparotid fascia is incised along the posterior facet of the parotid gland, and the parotid is retracted anteriorly and superiorly. Great care have to be exercised in dissecting and preserving the lower division of the facial nerve, which is generally the superior-most restrict of the exposure. To mobilize the hypoglossal nerve in the extra superior dissection, the descendens department should be minimize. Then the primary nerve may be retracted anterior and superior to the primary tumor dissection. Following the tumor resection, sequential closure of the deep muscle and fascia layers offers the best postoperative practical result. Patetsios and colleagues40 reported that of their 30 years of experience with carotid physique paragangliomas (29 sufferers with 34 tumors), problems included two arterial thromboses (7%), 5 everlasting cranial nerve deficits (17%), and one demise (3%). Labile blood strain, presumed to be secondary to baroceptor failure from lack of carotid sinus function, has been reported after resection of a carotid body tumor. Its prevalence in girls is way higher than in men, with an approximate 9: 1 ratio. Stanley and colleagues59 suggested that progestin and estrogen play a job in the improvement of the illness as a outcome of 94% of the sufferers they reviewed had been women. Likewise, the illness seems to contain primarily arteries with a paucity of vasa vasorum, indicating that arterial wall ischemia might contribute to illness progression. He reported a 71% mortality price associated to the aneurysm in untreated sufferers, in contrast with a 30% mortality in patients who underwent hunterian ligation. Treatment of those aneurysms evolved to attempts to protect the cerebral circulation and to avoid hunterian ligation. In the ensuing years, it grew to become clear that working on aneurysms in this location held only a slightly higher risk than a regular carotid endarterectomy when correct vascular methods have been used. The basic angiographic appearance, present in the more than 80% of patients, is the "string of beads"-multiple, irregularly spaced arterial constrictions with regular or ectatic intervening segments. Clinical Presentation the scientific signs related to extracranial carotid aneurysms vary according to their location and measurement. Large aneurysms often present as pulsatile cervical or parapharyngeal plenty that may or will not be tender.
Syndromes
- Septic shock
- An enlarged thyroid gland that contains nodules producing too much thyroid hormone (toxic nodular goiter)
- Infection
- Bone marrow biopsy
- Do not smoke.
- Slow weight gain
- Serum magnesium
- Excessive bleeding
Benemid 500mg discount line
The petrosectomy then becomes the cornerstone of a mix approach that relaxes the superior and posterior limitations myofascial pain treatment vancouver discount 500 mg benemid fast delivery. The two crucial additions are: (1) a supratentorial and infratentorial craniotomy that crosses the transverse sinus, and (2) division of the tentorium that gives communication between the supratentorial and infratentorial compartments pain treatment center franklin tn 500 mg benemid. Very little mind retraction is needed then to show the medial petrous and clival regions and associated neurovascular constructions. The entry, nonetheless, is proscribed however could also be modified by ligation and division of the sigmoid sinus. Translabyrinthine Approach the translabyrinthine publicity extends farther anterior than the retrolabyrinthine approach but nonetheless is finest suited to small aneurysms. The preliminary steps of this approach are the identical as the retrolabyrinthine method. These function bur holes for a subtemporal-suboccipital craniotomy that crosses the transverse sinus. Once the bone flap is removed, a big dural floor is exposed, and the transverse, sigmoid, and superior petrosal sinuses are seen. The mind is relaxed and the dura is incised anteriorly over the temporal lobe and curves posterior and inferior to the superior petrosal sinus under, where it enters the sigmoid sinus. A second dural incision is made inferiorly anterior to the sigmoid sinus, curving as a lot as the superior petrosal sinus. The superior petrosal sinus is split; the vein of Labb� is preserved when the dura is opened. Although not often needed, the sigmoid sinus can be sacrificed when the contralateral transverse and sigmoid sinuses are patent and communicate with the ipsilateral sinuses. If these angiographic and hemodynamic criteria are met, the sigmoid sinus can be divided beneath its confluence with the superior petrosal sinus. The vein of Labb� consistently enters the transverse sinus above this junction and so will drain contralaterally. Next, the tentorium is incised medially to the tentorial hiatus and posterior to the fourth nerve to connect the supratentorial and infratentorial compartments. The posterior temporal lobe is elevated with out traction on the vein of Labb�, which is tethered to the transverse sinus. This offers extensive exposure alongside the skull base from the foramen magnum to the dorsum sellae, with no use for brain retraction; the petrous area, clivus, brainstem, cranial nerves, and posterior circulation vessels now are seen easily. Extended Middle Fossa Approach the center fossa approach was developed to remove small, intracanalicular acoustic neuromas and protect the listening to apparatus. It is suitable for choose small basilar aneurysms as a outcome of the bony hall created is narrow and the fifth, seventh, and eighth nerves can restrict the view of the vertebrobasilar junction and reduce working area. For the process the patient is positioned supine, with the top positioned as for a subtemporal method. A query mark or horseshoe-shaped incision is used, and the pores and skin and temporalis muscle flaps are reflected anteriorly. A 5- � 5-cm craniotomy is made within the squamosal portion of the temporal bone, two-thirds anterior and one-third posterior to the external auditory canal. The center fossa floor is uncovered, the dura elevated medially to the petrous ridge, where a self-retaining retractor is positioned with its tip over the lip of the ridge. The combined supratentorial and infratentorial strategy is a mixture of the subtemporal and transpetrosal approaches. From this a craniotomy is made that crosses the transverse sinus and exposes the dura of the temporal lobe and cerebellum. B, the tentorium is split from the transverse-sigmoid junction to the incisura to reveal the cranial nerves, brainstem, clivus, and basilar artery. Next, the arcuate eminence that marks the underlying superior semicircular canal is recognized. As drilling proceeds laterally, the publicity is narrowed to keep away from the cochlea and superior semicircular canal. Once drilling is full, the petrous dural exposure extends from the superior to the inferior petrosal sinus. The superior petrosal sinus is coagulated and divided simply lateral to the trigeminal ganglion. The lower basilar artery can then be uncovered between the fifth and seventh nerves. The dura is opened in a Y-shaped trend, with care taken to control bleeding from the circular sinus. The cisterna magna arachnoid is opened, and the cervicomedullary junction is exposed. The vertebral arteries can be recognized anterior to the dentate ligaments coursing anteromedially. To achieve extra distal exposure, the interhemispheric fissure can be cut up between the tonsils. Far Lateral Approach the far lateral strategy provides extensive publicity of the vertebral trunk and anterolateral brainstem and is the most typical approach to vertebral trunk aneurysms35-37 because most are unilateral and lengthen beyond the area that can be accessed by way of a midline exposure. This creates a surgical hall alongside the vertebral artery axis that requires minimal cerebellar retraction. The outer cranial exposure is enhanced by resection of the C1 posterior arch and the posteroinferior skull base (including the posterolateral foramen magnum, posterior half of the occipital condyle, and jugular tubercle). The affected person could additionally be positioned in a lateral position, modified park bench or three quarters prone place with the lesion facet uppermost. The goal of positioning is to position the ipsilateral mastoid process on the highest point and maximally open the cervical-suboccipital angle. This places the clivus perpendicular to the ground to permit the surgeon to look down the axis of the vertebral and basilar arteries and to work between the horizontally arrayed cranial nerves. A hockey-stick incision is made that begins in the cervical midline over the C5 spinous process, extends cephalad to the inion, courses laterally along the superior nuchal line to the mastoid bone, and finishes inferiorly at the mastoid tip. The midline nuchal ligament is identified to separate the paraspinous musculature in this avascular aircraft. A minimize just below the superior nuchal line detaches the paraspinous muscles, that are mobilized inferolaterally to show the occipital bone and foramen magnum. This also creates a cuff for muscle reattachment throughout closure and mobilization quite than muscle transection and reduces postoperative ache. The vertebral artery as it programs from the transverse foramen of the C1 lateral mass, via the sulcus arteriosus of the C1 vertebral arch, to its dural entry level is identified and protected. The goal of bone removal is to show the angle between the lower medulla and cerebellum and scale back cerebellar retraction. There are three elements to bone removal: a C1 laminotomy, a lateral occipital craniotomy, and a condylectomy.
Benemid 500 mg purchase free shipping
Despite the success of preventive measures, injuries, together with unintentional accidents, homicide, and suicide, are the main explanation for dying within the United States and Europe in individuals youthful than forty five years cape fear pain treatment center lumberton nc 500 mg benemid purchase. Table 323-2 presents a abstract overview of reported incidence rates across the world treatment pain behind knee 500 mg benemid buy with visa. This latter figure may be very consistent with the 538 per 100,000 reported for the United States in a nationwide survey, together with emergency department visits, hospitalizations, and deaths. Some embody vacationers in a population-based analysis; others had been performed in comparatively small areas, which leads to a referral bias due to transport of extreme cases within the region. Population-based studies from Norway report an incidence of 229 per 100,000 in additional rural areas33 and eighty three. Slaughter and colleagues47 and Morrell and associates48 have indicated that a large share of persons detained in penal establishments report a history of head harm. An incidence of 17 per one hundred,000 together with a risk profile should lead to more effective preventive interventions. These information are primarily based on the outcomes of two large-scale epidemiologic investigations by certified neurologists and neurosurgeons. The comparatively low mortality at the side of the high prevalence and incidence present in these research would signify a substantial selection bias inflicting underneath reporting of mortality. Studies from Scandinavia have likewise proven a major lower in mortality from 1987 to 2001, which was extra pronounced in youthful patients, and the factor contributing to this lower is thought to be mainly the success of injury prevention efforts. In Australia, despite a 40% increase in population and a 120% improve in the number of registered automobiles, the amount of fatalities from highway incidents* decreased by 47% between 1970 and 1995. Most essential in these preventive measures seem like strict limits in blood alcohol focus, the use of seat belts and a separate baby restraint legislation, firmly enforced pace limits, and obligatory helmets for motorbike riders. Traffic fatality rates have increased by 44% in Malaysia, by up to 243% in China, and even by as a lot as 383% in Botswana. Consequently, maybe it might be better to target prevention campaigns in these nations not so much towards drivers however extra toward the overall inhabitants. In the United States, firearm injuries exceeded road site visitors incidents for the primary time in 1990, and this trend contrasted with the autumn in deaths from highway traffic incidents. A current Chinese study during which violent head trauma was analyzed in 11 hospitals over a 5-year period reported that 9. In this study, males and younger adults were most likely to maintain violent head trauma. Thoracic and stomach accidents have been typically lethal in the past, but more practical body armor has improved survival from these injuries considerably and resulted in an increased incidence of injuries in less protected areas, including the pinnacle. Blast injuries are now recognized as a separate entity; although the pathophysiology of blast injuries has not yet been properly characterized, prominent features of more extreme injuries are vasospasm and early brain swelling. The outcomes of aggressive management, together with early decompressive craniectomy, are encouraging. Frequently, refined and transient symptoms are reported, they usually might overlap with signs caused by posttraumatic stress disorders and postconcussion syndromes. Likewise, others may include patients reporting some mental complaints after damage CauseofInjury the primary causes of neurotrauma are transportation incidents, falls, and gunshot wounds. These injuries, brought on by misadventure, violence, or carelessness, all replicate societal conduct. Gilbert acknowledged that the motorcar "had emerged as essentially the most persistent killer within the western world. In contrast, many road traffic injuries are preventable and will due to this fact not be categorized as accidents. Whether these variations symbolize beneath reporting in the United Kingdom or over-reporting in the United States stays a matter of speculation. More importantly, a rise in amenities for long-term therapy and care will be needed. Neurotrauma is a selected burden in developing international locations, which have the least capacity to handle it. Successful prevention and reduction of the incidence of neurotrauma can happen solely with higher political motion, public consciousness, and the participation of societies. Kannus and colleagues showed an increase in fallinduced head harm over time from 1970 to 1995, even after correction for demographic changes. In this regard, it ought to be remembered that an elderly affected person maintained on anticoagulant remedy in whom an acute subdural hematoma develops after an initial lucid interval is similar to a youthful patient with an epidural hematoma (and secondary mind compression) from a pathophysiologic perspective. We evaluation the first mechanical forces that contribute to those mind accidents, how these mechanical forces trigger motion and harm throughout the brain, and the out there information on tips on how to forestall most of these accidents. This information is offered as an introduction solely, and more detailed investigations of those rules could be found in other publications. Skull fracture might or could not involve injury to the underlying brain, however the fracture is usually not a direct cause of neurological incapacity. Focal injuries happen in almost half of all sufferers with severe mind damage and are answerable for approximately two thirds of mind injury�related deaths. In its mildest form (concussion), diffuse brain damage could not essentially be structural and may contain solely alterations in neural excitability, neurotransmission, or long-term changes in receptor dysfunction and associated disabilities. In extra extreme circumstances, diffuse brain injury is manifested as extended coma and not using a mass lesion and entails some degree of structural derangement on the microscopic level. Diffuse mind harm might sometimes include secondary damage from both brain swelling and ischemic injury. Static or quasi-static loading is an unusual occurrence and is used to explain a scenario during which force is applied to the head very slowly, typically occurring over times longer than 200 msec. Squeezing or crushing of the skull generally occurs on account of this static or quasi-static loading, as seen in earthquakes, constructing collapses, or equipment accidents, and it includes fractures at the vault or basilar skull area. At excessive ranges of drive, the severe compression of the brain can result in herniation of the brain contents and frequently deadly mind harm. Dynamic loading is the more frequent kind of mechanical loading to the head, particularly when one considers traumatic injury. Impulsive loading happens when the head is about into motion indirectly by a blow to a different body region, similar to when a running again is hit within the midtorso by a heavy lineman in American soccer or the sudden movement of an unrestrained head when the torso is restrained throughout a vehicular crash. The resulting inertial force utilized to the pinnacle causes the brain to maneuver within the cranium; the nature and interaction of this mind movement with the inner cranium constructions results in damage alongside the brain surface and inside the brain parenchyma. Fifty-one average to severe head accidents occurred during the interval 1996 to 2003 in vehicle racing drivers who have been exposed to high acceleration throughout crashes without the top or face making direct contact. In the worst instances, fatal basilar cranium fracture was seen with cranial-cervical distraction. Another example of impulse loading without the head sustaining direct contact is the mind harm that results from "shaken baby syndrome. Impact loading is advanced and normally results in a mix of contact drive and inertial (head motion) force.
500 mg benemid buy with visa
Do not us e wi th etha nol or protei n hydrol ys a tes, preci pi ta ti on ma y type back pain treatment nhs purchase benemid 500 mg on-line. If a dvers e rea cti ons (eg, fever, ta chyca rdi a, hypotens i on, or dys pnea) occur, i nfus i on s houl d be s topped a nd pres cri ber noti fi ed neuropathic pain treatment 500 mg benemid overnight delivery. Bronchos pa s m (trea tment): Ora l: 2 mg 3-4 ti mes /da y; ma xi mum: eight mg four ti mes /da y Dos i ng: Pedi a tri c Bronchospasm: Oral, regular release: Chi l dren 2-6 yea rs: zero. Sol uti on for nebul i za ti on: Concentra ted s ol uti on s houl d be di l uted pri or to us. Di eta ry Cons i dera ti ons Ora l forms s houl d be a dmi ni s tered wi th wa ter 1 hour earlier than or 2 hours a fter mea l s. Ta bl et, extended rel ea s e: Store a t 20�C to 25�C (68�F to 77�F) Recons ti tuti onSol uti on for nebul i za ti on: To prepa re a 2. Dos i ng: Pedi a tri c Antiseptic:Liquid denatured alcohol: Refer to a dul t dos i ng. Treatment of methanol or ethylene glycol ingestion (unlabeled use):Absolute ethanol/ethyl alcohol: Refer to a dul t dos i ng. Treatment of fat occlusion of central venous catheters (unlabeled use):Dehydrated alcohol injection: Refer to a dul t dos i ng. Risk X: Avoid combination Amprena vi r: Al cohol (Ethyl) ma y enha nce the a dvers e/toxi c effect of Amprena vi r. Risk X: Avoid mixture Cefa ma ndol e: Ma y enha nce the a dvers e/toxi c impact of Al cohol (Ethyl). Risk C: Monitor therapy Cefoteta n: Ma y enha nce the a dvers e/toxi c impact of Al cohol (Ethyl). Risk C: Monitor remedy Di s ul fi ra m: Ma y enha nce the a dvers e/toxi c impact of Al cohol (Ethyl). Risk X: Avoid combination Fura zol i accomplished: Ma y enha nce the a dvers e/toxi c impact of Al cohol (Ethyl). Risk C: Monitor therapy Gri s eoful vi n: Ma y enha nce the a dvers e/toxi c effect of Al cohol (Ethyl). Risk C: Monitor therapy Sul fonyl urea s: Ma y enha nce the a dvers e/toxi c effect of Al cohol (Ethyl). Pha rma codyna mi cs /Ki neti cs Abs orpti on: Ora l: Ra pi d Di s tri buti on: Vd: zero. Ameri ca n Aca demy of Pedi a tri cs Commi ttee on Drugs," Pediatrics, 1998, 101(6):1079-88. Admi ni s tra ti on: OtherMa y be a dmi ni s tered by SubQ i njecti on (unl a bel ed route). Final Dilution Concentration Final Dilution Concentration Stability (mcg/mL) (106 int. Concerns related to opposed effects: � Advers e results: Are frequent a nd s ometi mes fa ta l. Boxed Warning]: Impaired neutrophil perform is associated with remedy; sufferers are at risk for sepsis, bacterial endocarditis, and central line-related gram-positive infections. Boxed Warning]: Withhold therapy for patients developing moderate-to-severe lethargy or somnolence; continued treatment might lead to coma. Boxed Warning]: Should be administered beneath the supervision of an skilled cancer chemotherapy doctor in a facility with cardiopulmonary or intensive specialists and intensive care services available. Risk C: Monitor remedy Interferons (Al fa): Ma y enha nce the a dvers e/toxi c effect of Al des l euki n. Fol l owi ng recons ti tuti on, ma y be s tored for up to four hours a t 2�C to 8�C (36�F to 46�F). Cons i der premedi ca ti ng wi th di phenhydra mi ne 50 mg a nd a ceta mi nophen 5001000 mg 30 mi nutes before i ni ti a ti on of i nfus i on. Boxed Warning]: Severe, extended myelosuppression, autoimmune anemia, and autoimmune thrombocytopenia have occurred. Di s conti nue thera py duri ng s eri ous hema tol ogi c or other s eri ous toxi ci ty (except l ymphopeni a) unti l the event res ol ves. Boxed Warning]: Serious infections (bacterial, viral, fungal, and protozoan) have been reported. Wi thhol d trea tment duri ng s eri ous i nfecti ons; ma y be rei ni ti a ted upon res ol uti on of i nfecti on. Special populations: � Men of reproducti ve potenti a l: Shoul d us e effecti ve contra cepti ve strategies duri ng trea tment a nd for a mi ni mum of 6 months fol l owi ng thera py. Nurs i ng: Phys i ca l As s es s ment/Moni tori ngSee Wa rni ngs /Preca uti ons a nd Contra i ndi ca ti ons for extens i ve us e ca uti ons. Stora geStore a t 20�C to 25�C (68�F to 77�F); excurs i ons permi tted to 15�C to 30�C (59�F to 86�F). Drug Intera cti ons Ami nogl ycos i des: Ma y enha nce the hypoca l cemi c impact of Bi s phos phona the Deri va ti ves. Risk D: Consider remedy modification As pi ri n: Ma y enha nce the a dvers e/toxi c impact of Al endrona te. If extra cti ons were ca rri ed out, the ca l cul a ted frequency wa s 1 i n 1130 to 1 i n 296 (0. Al fenta ni l Approx Duration of Anesthesia (min) Induction Period (Initial Dose) (mcg/kg) Maintenance Period (Increments/ Infusion) Indication Total Dose (mcg/kg) Effects 30 8-20 3-5 mcg/kg or zero. Disease-related issues: � Bra dya rrhythmi a s: Us e wi th ca uti on when a dmi ni s teri ng to pa ti ents wi th bra dya rrhythmi a s. Risk D: Consider therapy modification Anti ps ychoti c Agents (Phenothi a zi nes): Ma y enha nce the hypotens i ve effect of Ana l ges i cs (Opi oi d). Risk C: Monitor therapy Propofol: Al fenta ni l ma y enha nce the a dvers e/toxi c impact of Propofol. Risk D: Consider therapy modification Beta -Bl ockers: Ma y enha nce the orthos ta ti c impact of Al pha 1-Bl ockers. Risk D: Consider therapy modification Ta ms ul os i n: Al pha 1-Bl ockers ma y enha nce the a nti hypertens i ve effect of Ta ms ul os i n. Risk X: Avoid mixture Etha nol /Nutri ti on/Herb Intera cti ons Food: Food i ncrea s es the extent of a bs orpti on. Moni tori ng Pa ra meters Uri ne fl ow; bl ood pres s ure Nurs i ng: Phys i ca l As s es s ment/Moni tori ngPros ta ti c ca rci noma s houl d be rul ed out earlier than begi nni ng thera py. Pha rma codyna mi cs /Ki neti cs Abs orpti on: Decrea s ed 50% under fa s ti ng condi ti ons Di s tri buti on: Vd: three. Concomi ta nt us e wi th ps ychotropi cs ma y produce a ddi ti ve results on bl ood pres s ure. Once di l uted, 100 mL a nd 200 mL s ol uti ons for i nfus i on a re s ta bl e for 18 hours when s tored a t 2�C to 8�C. Boxed Warning]: Severe hypersensitivity reactions, together with anaphylactic reactions and anaphylactic shock have been reported during infusion. Us e ca uti on wi th s ubs equent i nfus i ons; i nfus i on rea cti ons ha ve occurred des pi the premedi ca ti on wi th a nti hello s ta mi nes, a nti pyreti cs, a nd/or s teroi ds. Premedi ca ti on wi th a nti hello s ta mi nes a nd/or a nti pyreti cs ma y be ordered. Pha rma codyna mi cs /Ki neti cs Di s tri buti on: Vss: 80-112 mL/kg Ha l f-l i fe el i mi na ti on: 2.
Order benemid 500mg
Multicenter evaluate of preoperative threat factors for endarterectomy for asymptomatic carotid artery stenosis pain treatment wiki 500 mg benemid generic with visa. Long-term results of carotid stenting versus endarterectomy in high-risk patients neuropathic pain treatment guidelines australia buy benemid 500 mg on-line. Frequency and administration of recurrent stenosis after carotid artery stent implantation. Advancements in carotid stenting resulting in reductions in perioperative morbidity among sufferers 80 years and older. LeRoux Blunt harm to the carotid or vertebral vessels (blunt cerebrovascular injury) is unusual and is identified in about 1 of 1000 (0. Consequently, the mortality and morbidity related to blunt cerebrovascular damage are often excessive. This chapter critiques the pathology, clinical presentation, imaging, diagnosis, and treatment of blunt carotid and vertebral artery injuries. The chapter focuses on carotid artery injuries, but distinctive elements of vertebral artery accidents are additionally reviewed. There is a paucity of specific suggestions for blunt cerebrovascular damage in kids. In explicit, blunt vascular injuries happen with cervical hyperextension and rotation, hyperflexion, or a direct blow. The carotid arteries are motionless on the skull base, and the traumatic movement stretches the carotid artery over the higher cervical vertebrae and tears the vessel intima. Other mechanisms of blunt carotid injury embrace strangulation, basilar skull fractures, and facial fractures. Extradural vertebral artery dissections or accidents are associated with cervical backbone fractures, notably these with a rotational element. The carotid or vertebral artery often might undergo iatrogenic damage throughout neurosurgical or angiographic procedures that involve vessel exposure, passage of hardware near or via the artery, or direct manipulation of the vessel. In specific, harm may occur where a cellular vessel segment traverses a set location, such because the cranium base foramina. The vertebral artery is mobile in its proximal (V1) and distal (V3) extradural segments. Intradural vertebral artery accidents (V4) might occur from extension from the V3 segment. The risk for harm could also be increased among sufferers with certain connective tissue problems, similar to fibromuscular Pathologic Findings Arterial walls are composed of three layers: an inner or endothelial layer (tunica intima), a middle or muscular layer (tunica media), and an exterior or connective tissue layer (tunica adventitia). Dissection is a typical manifestation of blunt damage and usually results from a tear or disruption of the intima. This tear starts a cascade of occasions that features subintimal publicity causing platelet adherence and a website for thrombus formation and embolization. Extradural accidents due to this fact are much less prone to trigger hemorrhage until the injury is within the cranium base cavities. Ischemic signs (embolic or hypoperfusion) due to this fact are extra frequent after extradural injuries, whereas aneurysm enlargement and hemorrhage (subarachnoid hemorrhage) are extra frequent with intradural lesions. This could slender or occlude the lumen, significantly if positioned between the intimal and medial layers and thus causing hypoperfusion. Intramural hematomas additionally compromise the structural integrity of the vessel wall, so a traumatic aneurysm occurs significantly when the hematoma extends between the medial and adventitial layers. When the walls of the dilated aneurysmal segment are composed of the incomplete remaining parts of the vessel, a dissecting aneurysm varieties. Complete disruption of the arterial wall results in blood extravasation into the encompassing buildings. In extradural areas, the hemorrhage is into delicate tissue, and a pseudoaneurysm forms. Dissecting aneurysms may continue to speak with flowing blood, and subsequently delayed progress may occur. Alternatively, because of slow move within the aneurysm, intraluminal thrombosis occurs, resulting in embolization. In the awake patient, extreme unilateral headache might precede neurological signs; nonetheless, ischemic signs tend to develop quickly. The affected person could present with acute signs or in a subacute fashion, or symptoms could develop in a delayed style (hours to weeks). In addition, many patients with blunt cerebrovascular injuries are completely asymptomatic. Risk factors for vertebral artery accidents embody cervical backbone fractures, significantly these associated with severe flexion or extension; upper cervical backbone injuries; and fractures by way of the foramen transversarium. Extradural Vertebral Artery Injury In the conscious patient, headache or neck ache is the most common presentation of extradural vertebral artery damage. Lateral medullary infarction is the most common stroke brought on by extradural vertebral artery damage or dissection. Intradural Vertebral Artery Injury Headache and fewer generally vertigo, tinnitus, nausea, and vomiting are the usual symptoms in the awake affected person. Lateral medullary syndrome is the most typical stroke, though other strokes that contain the brainstem may happen. Physical Findings On physical examination, patients may current with a neck hematoma, bruits, pulsatile neck mass, or a palpable thrill (Table 352-1). Extradural Carotid Injury Nonspecific headache is a common presentation of blunt carotid injury within the awake trauma affected person. In some collection of blunt cerebrovascular accidents, this is how 18% to 34% of sufferers current. A, Serial axial computed tomography photographs demonstrating a fracture that entails the cranium base round the proper inside carotid artery. Furthermore, noninvasive imaging suggests rather than confirms the prognosis of intradural dissection. In contrast to its major function within the evaluation of extradural dissections, noninvasive imaging typically suggests rather than confirms the analysis of intradural dissection. Magnetic resonance angiography (B) and digital subtraction angiography (C) reveal a left inside carotid artery dissection. Angiography Angiographic examination of suspected blunt cerebrovascular injury requires a four-vessel angiographic study. Radiographic features to look at on intracranial views embrace intradural extension of an extradural dissection and evidence of emboli, collaterals, slow circulate, or stagnation of distinction. The stenosis of dissection differs in its configuration and location from that seen with atherosclerotic disease. Most typically, dissection-related occlusion demonstrates a tapered or flame-shaped distal extent in the acute phase.
Inositol Monophosphate (Inositol). Benemid.
- How does Inositol work?
- Problems metabolizing fat, high cholesterol, inability to sleep, attention deficit-hyperactivity disorder (ADHD), cancer, hair growth, and other conditions.
- Autism.
- Are there safety concerns?
- Dosing considerations for Inositol.
- Schizophrenia.
- Depression.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96321
500 mg benemid order overnight delivery
In patients with symptomatic ischemia from vessels narrowing as a end result of dissection or embolic occasions regardless of anticoagulant remedy, surgical or endovascular intervention is indicated who pain treatment guidelines buy benemid 500mg on line. Direct surgical restore of the dissection in seldom possible, although surgical choices embrace both a superficial temporal artery�to�middle cerebral artery bypass or a high-flow saphenous vein graft bypass, relying on the necessity for cerebral blood flow heel pain treatment webmd benemid 500 mg cheap free shipping. An endovascular possibility is available even in patients with high cervical dissections. Angioplasty and stenting stay viable options, whilst main treatment issues. In complex instances or dissections resulting in a double lumen, the problem lies in identifying which is the true lumen and which is the false one. Provided the stent is properly apposed to the lumen wall, small pseudoaneurysms or vessel irregularities outdoors the stent typically thrombose with time, even when sufferers are receiving antiplatelet medical remedy. In a sequence of 26 consecutive sufferers with carotid dissection handled with angioplasty and stenting, Kadkhodayan and coworkers113 reported that dissection-induced stenosis was lowered from 71% � 18% to no significant stenosis in 95% of patients. In sufferers with complete occlusions from spontaneous dissections who have been treated with anticoagulation remedy, the long-term recanalization rate was 47% within the report by Pozzati and coworkers110,111 and 43% in that by Bogousslavsky and associates. In 1899, Gassman described histologically the small vessel endothelial proliferation associated with radiodermatitis. In 1944, Sheehan121 reported a extra detailed study during which he described the event of plaque-like thickenings within the intima of small arteries secondary to the accumulation of froth cells, hyaline, and fibrin within the endothelial lining and internal elastic membrane. This dysfunction leads to lysosomal activation and cellular proliferation within the vessel wall, resulting in intimal plaque formation. With the expanded use of radiation within the therapy of neck and mediastinal malignancies, reports of radiation modifications in larger arteries grew to become extra prevalent. In 1940, Cade123 briefly mentioned a case of presumed radiation injury to the aorta of a patient handled for esophageal most cancers. Thomas and Forbus,124 nonetheless, are credited with the first medical report of a affected person with radiation injury in a big artery. In 1959, they detailed the course of a 19-year-old patient who underwent radiotherapy for mediastinal lymphoma. Imaging studies are indicated for patients who developed symptoms of cerebral ischemia or emboli after radiotherapy to the top, neck, or mediastinum. Third, some authors speculate that the carotid arterial wall is damaged, making carotid endarterectomy in these sufferers extra dangerous than a regular carotid endarterectomy. Magnetic resonance angiography of the arteries can give a extra complete view of the arterial origins in excessive cervical segments127 however will not be obtainable in some patients. Cervical and cerebral angiography remains the "gold commonplace" for evaluating potential radiation stenosis. Two thirds of the patients had extreme scarring or fibrosis of the pores and skin of the neck, and 4 patients had permanent tracheostomies. Complications have been limited to 2 restenoses, two wound infections, and four cranial nerve palsies. A patch graft arterial repair was needed in 79% of the surgically handled patients. Endovascular remedy can additionally be a viable possibility in the treatment of radiation stenosis of the carotid arteries. Because of issues related to soft tissue fibrosis, operating via an area of a earlier myocutaneous flap, and more proximal arterial involvement, endovascular angioplasty stenting has emerged as the primary treatment for radiation stenosis. The long-term efficacy of stenting on this setting has yet to be analyzed, however the shortterm outcomes are promising. The 30-day postprocedure complication fee was zero of 23 (0%), and no new neurological signs have been reported. With a imply follow-up time of 28 months (range, 5 to seventy eight months), 15 of the 19 vessels (79%) developed no new stenosis, 2 of 19 (11%) had repeat angioplasty and stent placement, and 1 of 19 (5%) had a repeat angioplasty. Finally, preliminary outcomes from controlled, potential randomized trials of carotid angioplasty and stenting in highsurgical-risk sufferers appear promising. Carotid physique tumors, inheritance, and a excessive incidence of associated cervical paragangliomas. Angioplasty and stenting in carotid dissection with or with out associated pseudoaneurysm. Some morphological histochemical, and chemical observations on chemodectomas and the traditional carotid body, including a examine of the chromaffin reaction and attainable ganglion cell components. Fibromuscular dysplasia: neurological disorders related to disease involving the nice vessels in the neck. Subsequently, in 1853, Maisonneuve efficiently ligated the vertebral artery on the transverse foramen of the sixth cervical vertebra for a stab wound to the neck. In 1888, Matas2 was the primary surgeon who totally excised an aneurysm between the occiput and the atlas through a posterior method. The function of pathology of the extracranial vessels in relation to cerebral ischemia was emerging,5 and with this revolution in the diagnosis of diseased arteries, revascularization was being carried out. In 1958, Crawford and coworkers6 offered their outcomes of surgical remedy of brainstem ischemia by reconstructing the vertebral artery after eradicating atherosclerotic plaque. The subsequent yr, Cate and Scott7 first described the technique of transsubclavian endarterectomy of the subclavianvertebral artery. Angiography allowed visualization of other causes of extracranial vertebral artery disease, including extrinsic compression of the vertebral artery by osteophytes,eight constricting bands,9 and rotational obstruction,10 all of which had been recognized and treated by surgical decompression. Angiography additionally provided the primary in depth cooperative examine of the incidence of extracranial arterial stenosis attributable to atherosclerotic lesions in sufferers with cerebrovascular insufficiency. In 1968, stenosis was proposed to be a compromised lumen of more than 50% by the Joint Study of Extracranial Arterial Occlusion. For the primary time, this research offered a frequency distribution of sites of stenosis within the extracranial vertebral artery,eleven identifying no much less than some degree of stenosis in 22% and 18% of left and right proximal vertebral arteries, respectively, and 5% to 6% of the distal extracranial vertebral. Today, posterior circulation stroke nonetheless accounts for 30% to 40% of all ischemic strokes, a subset of which is secondary to isolated extracranial vertebral artery disease. Treatment options have advanced to incorporate endovascular choices, though surgical intervention remains a valid option for extracranial vertebral artery revascularization in plenty of instances. Most physicians use the presence of any two of the common signs to define the syndrome. The designation is helpful because the related pathology can differ among the many segments. First Vertebral Artery Segment (V1) the V1 extends from the superior portion of the subclavian artery to enter the transverse foramen of C6. Instead of arising from the superior portion of the left subclavian artery, the left vertebral artery can arise from the proximal subclavian trunk. These signs are brought on not only by embolic or thrombotic sources but also by hemodynamic mechanisms. As the vertebral artery enters the transverse foramen of C6, it ascends in a vertical path through the higher cervical foramen until it approaches C2. From the C2 transverse foramen, it programs slightly anteriorly to pass through the transverse foramen of C1. This segment can be extremely tortuous, which makes the endovascular placement of a stent in the mid or the distal extracranial vertebral artery troublesome.
Buy 500mg benemid mastercard
Nurs i ng: Phys i ca l As s es s ment/Moni tori ngSee i nforma ti on rel a ted to s ki n tes ts a nd des ens i ti za ti on dna advanced pain treatment center pa benemid 500 mg discount amex. In event of hypers ens i ti vi ty or hypergl ycemi a, i nfus i on s houl d be s topped a nd pres cri ber noti fi ed i mmedi a tel y pain medication for dogs with bone cancer 500mg benemid purchase with mastercard. Risk C: Monitor remedy Sel ecti ve Serotoni n Reupta ke Inhi bi tors: Ma y enha nce the a nti pl a tel et impact of As pi ri n. Stora geStore a t 25�C (77�F); excurs i ons permi tted to 15�C to 30�C (59�F to 86�F). Risk C: Monitor therapy Adenos i ne: Di pyri da mol e ma y enha nce the thera peuti c effect of Adenos i ne. Risk D: Consider remedy modification Al endrona te: As pi ri n ma y enha nce the a dvers e/toxi c effect of Al endrona te. Risk C: Monitor remedy Ibri tumoma b: Anti pl a tel et Agents ma y enha nce the a dvers e/toxi c effect of Ibri tumoma b. Risk C: Monitor therapy Rega denos on: Di pyri da mol e ma y enha nce the thera peuti c effect of Rega denos on. Risk D: Consider therapy modification Hepa ri n: As pi ri n ma y enha nce the a nti coa gul a nt effect of Hepa ri n. Risk C: Monitor remedy Ketorol a c: Ma y enha nce the a dvers e/toxi c effect of As pi ri n. Ameri ca n Col l ege of Obs tetri ci a ns a nd Gynecol ogi s ts," Int J Gynaecol Obstet, 2002, 77(1):67-75. Note: Trea tment-na i ve pa ti ents 39 kg a nd thirteen yea rs of a ge who a re una bl e to tol period the ri tona vi r, check with a dul t dos i ng. Di eta ry Cons i dera ti ons Shoul d be ta ken wi th food to enha nce a bs orpti on. Advers e Rea cti ons Incl udes da ta from each trea tment-na i ve a nd trea tment-experi enced pa ti ents. Na us ea, di zzi nes s, hypotens i on, a nd s yncope ha ve been reported wi th concomi ta nt us e of tra zodone a nd ri tona vi r. Ca l cul a ti ons Crea ti ni ne Cl ea ra nce: Adul ts Admi ni s tra ti on: Ora l Ma y be a dmi ni s tered wi thout rega rd to mea l s. Risk D: Consider therapy modification Ami oda rone: Ma y enha nce the bra dyca rdi c effect of Beta -Bl ockers. The i njecti on ca n be a dmi ni s tered undi l uted or di l uted wi th a compa ti bl e I. Do not a djus t dos a ge or di s conti nue medi ca ti on wi thout cons ul ti ng pres cri ber. Mul ti middle Study of Peri opera ti ve Is chemi a Res ea rch Group," N Engl J Med, 1996, 335(23):1713-20. Boxed Warning]: Use with caution in pediatric sufferers; could also be an increased danger of suicidal ideation. Risk C: Monitor remedy Beta 2-Agoni s ts: Atomoxeti ne ma y enha nce the ta chyca rdi c impact of Beta 2-Agoni s ts. Appea ra nce of s ymptoms must be i mmedi a tel y reported to hea l thca re provi der. A Compa ri s on of Atorva s ta ti n, Si mva s ta ti n, Lova s ta ti n, a nd Fl uva s ta ti n," Pharmacoeconomics, 1998, 14(1):59-70. Atorva s ta ti n Vers us Reva s cul a ri za ti on Trea tment Inves ti ga tors," N Engl J Med, 1999, 341(2):70-6. Herb/Nutra ceuti ca l: Herbs wi th hypogl ycemi c properti es ma y enha nce the hypogl ycemi c impact of a tova quone. Report unres ol ved di a rrhea, fever, mouth s ores (us e good mouth ca re), unres ol ved hea da che, or vomi ti ng. Compatibility in syringe: Compatible: Al fenta ni l, fenta nyl, mi da zol a m, s ufenta ni l. Risk C: Monitor therapy Ketorol a c: Ma y enha nce the a dvers e/toxi c effect of Neuromus cul a r-Bl ocki ng Agents (Nondepol a ri zi ng). Sa fety preca uti ons mus t be ma i nta i ned unti l ful l mus cl e tone ha s returned. Emergency medi ca l pers onnel who ha ve s el f-a dmi ni s tered a dos e mus t determi ne ca pa ci ty to conti nue to provi de ca re. Chi l dren ma y be more s ens i ti ve to the a nti chol i nergi c results of a tropi ne. In a ddi ti on, ti me i nterva l to "a gi ng" proces s (i rrevers i bl e bi ndi ng between orga nophos pha tes a nd a cetyl chol i nes tera s e) va ry dependi ng on nerve a gent. If a tropi ni za ti on occurs a fter 1-2 mg of a tropi ne then re-eva l ua the worki ng di a gnos i s. Mydriasis, cycloplegia (preprocedure):Ophthalmic (1% s ol uti on): Ins ti l l 1-2 drops 1 hour earlier than the process. Prehospital ("within the subject"): Bi rth to <2 yea rs: Mi l d-to-modera the s ymptoms: zero. Compatibility in syringe: Compatible: Butorpha nol, chl orproma zi ne, ci meti di ne, di menhydri na te, di phenhydra mi ne, droperi dol, fenta nyl, gl ycopyrrol a te, hepa ri n, hydromorphone, hydroxyzi ne, hydroxyzi ne wi th meperi di ne, meperi di ne, meperi di ne wi th prometha zi ne, metocl opra mi de, mi da zol a m, mi l ri none, morphi ne, na l buphi ne, onda ns etron, penta zoci ne, perphena zi ne, prochl orpera zi ne, proma zi ne, prometha zi ne, propi oma zi ne, ra ni ti di ne, s copol a mi ne, s ufenta ni l. Compatibility when admixed: Compatible: Dobuta mi ne, furos emi de, meropenem, s odi um bi ca rbona te, vera pa mi l. Atropi ne ha s no impact on the ni coti ni c receptors res pons i bl e for mus cl e wea knes s, fa s ci cul a ti ons, a nd pa ra l ys i s. Dos i ng: Pedi a tri cDiarrhea: Ora l (gi ve a fter ea ch bowel movement): Chi l dren: 3-6 yea rs: 300 mg/dos e; ma xi mum dos e: 2100 mg/da y 6-12 yea rs: 600-750 mg/dos e; ma xi mum dos e: 4500 mg/da y Chi l dren >12 yea rs: Refer to a dul t dos i ng. Geri a tri c Cons i dera ti ons El derl y often pres ent bowel i mpa cti on wi th di a rrhea. Pha rma codyna mi cs /Ki neti cs Abs orpti on: Not a bs orbed Rel a ted Informa ti on Bi s muth Pha rma cothera py Pea rl s Atta pul gi the ha s been faraway from the U. Other warnings/precautions: � Moni tori ng: La bora tory moni tori ng s houl d be compl eted pri or to ea ch new pres cri pti on. N-a cetyl cys tei ne Trea tment of Hema tol ogi c Rea cti ons to Chrys othera py," J Rheumatol, 1982, 9(4):519-26. Report of Two Ca s es a nd Revi ew of the Li tera ture," Rev Clin Esp, 1995, 194:540-2. Infus e over 10-40 mi nutes; i nfus i on mus t be compl eted wi thi n 1 hour of (vi a l) recons ti tuti on. Al l ow refri gera ted s us pens i ons to come to room tempera ture (up to 30 mi nutes) pri or to a dmi ni s tra ti on. Admi ni s tra ti on mus t be compl eted wi thi n 1 hour of (vi a l) recons ti tuti on. Renal transplantation, rheumatoid arthritis (unlabeled uses): Refer to a dul t dos i ng.
Benemid 500mg buy discount line
However, because of the infrequency of pure rotational motions in scientific conditions, the results of rotational acceleration are usually seen after angular acceleration of the head uab pain treatment center benemid 500 mg buy without prescription. Angular acceleration occurs when components of translational and rotational acceleration are mixed pain treatment shingles 500 mg benemid cheap with visa. The precise location of this rotation point, in conjunction with the magnitude of the impression drive, determines the proportion of translation and rotation that the mind experiences. As might be expected, angular acceleration is essentially the most damaging brain damage mechanism as a result of it combines the injurious mechanism of both translational and rotational movements, especially the latter. Virtually each known type of head injury could be produced by angular acceleration, apart from cranium fracture and epidural hematoma. Several studies have now documented the in vivo motion of the mind throughout angular motions13,14 and have investigated the top motions associated with sports and concussive impacts. Itisraretofindinstances of pure translational or rotational acceleration in "real-world" damage situations. The angular movement results in combined translational and rotational acceleration, thereby creating injury patterns that arise from each acceleration types. The quantity of inertially induced harm relies upon not only on the kind of acceleration imparted to the top but additionally on several different components. The magnitude of acceleration could be considered as being proportional to the quantity of strain delivered to the mind, and the acceleration price is proportional to the strain rate. Both pressure and the pressure price are components contributing to the structural or functional limit of intracranial tissues. If the magnitude of acceleration is fixed, the rate of acceleration varies inversely with the duration for which the acceleration is applied. Acceleration magnitude Blast-Induced Brain Injuries the results of blast loading on humans originated with the term "shell shock" from World War I, which was used to describe a group of symptoms that included a temporary altered psychological state or confusion immediately after the blast. Despite being periodically addressed since its recognition as a medical syndrome, solely very current studies have better described the circumstances of blastinduced brain injury. The main damage part consists of the response of brain tissue to the blast wave (an intense overpressurization impulse part of the blast). The tertiary damage phase is due to head contact/acceleration because the body is moved by the "blast wind" (forced super-heated airflow). These groupings apply to the examine of not solely brain injuries but additionally different physique areas susceptible to injury from blast. Primary blast damage is restricted to accidents caused by the quickly increasing blast wave. In air, the shock wave oscillates between overpressure and underpressure segments, but these waves dampen out rapidly. The presence of structures and fluid interfaces complicates this stress profile. Studies in these areas have generated injury thresholds for each the pulmonary system and the gut/bowel. Secondary blast injury covers each the penetrating and nonpenetrating injuries that occur when high-velocity projectiles/ fragments impression the pinnacle. Conversely, if the period of acceleration is fixed, the acceleration fee varies directly with the magnitude of the acceleration. If one applies a continuing quantity of acceleration and varies solely the duration over which the acceleration occurs, three zones of medical curiosity are encountered. The actual relationships between mechanical loading (magnitude, kind, and course of acceleration) and damage patterns are becoming more and more more refined with computational fashions of the head/brain construction. Second, if the duration of acceleration is slightly longer, strain begins to appear within the mind but is primarily restricted to the periphery. Injuries produced in these circumstances are confined to the brain periphery and vessels. It is thus extremely complicated to try to map acceleration profiles into actual patterns of harm within the brain. Several easy descriptors of acceleration-the amount and type of acceleration, its length, and the speed at which the acceleration is applied to the head-are interrelated and together contribute to the pattern of injury observed within each individual. Certainly, these parameters are linked; for instance, with a continuing level of acceleration, because the length increases, head velocity and movement additionally enhance. A exhausting impacting object can cause a linear fracture, with many of the vitality from the object getting used to deform the skull domestically. To prevent a more localized depressed cranium fracture, the impacting object should be larger than roughly 2 square inches. However, if the impacting object or surface is significantly bigger, the contact is distributed across a broad space of the scalp and the local bending effects needed for fracture to happen will not be current. Acceleration injuries might occur in parallel with an influence that will trigger a fracture because most influence conditions will set the pinnacle in movement and therefore cause acceleration of the head superimposed on the contact loading effects. Management of the power of the influence for a cranium fracture occurs instantly beneath the impactor. If the impacting force is substantial, all bone underneath the impactor is broken and cranium perforation happens. Nevertheless, the mechanics of these penetrating lesions is becoming clearer, given the frequency of gunshot wounds in the civilian inhabitants. This induces cavitation damage along the path of the projectile, as properly as primary laceration injury alongside the trail of the fragment. At the mechanistic stage, these accidents are finest modeled as a tissue laceration, with the plain complicating mechanisms related to blood within the extracellular area and the potential for secondary mind accidents similar to hypoxia. Tertiary blast injury happens when the first blast wind causes the victim to collide with fastened or mobile objects. These kinds of injuries share probably the most in frequent with contact/ acceleration accidents in civilians, where both the contact and acceleration forces can contribute to the totally different intracranial injuries that occur. Helmets worn by troops reduce the likelihood of accidents from direct contact for many of the head. As a outcome, the predominant mechanism of tertiary blast injuries in helmeted troops is the intracranial deformations caused by the top hanging an object or the pinnacle being struck by an object with adequate mass to trigger a significant inertial load. In nonhelmeted victims, tertiary blast injuries can even embody skull fracture or contusions from focal contact forces when the unprotected head strikes an object or floor. Basilar Fracture Caused mainly by either direct impact or propagation of stress waves through the cranium as a end result of distant impression, basilar fractures can also occur as a consequence of the impression to facial bones. The skinny anterior basilar cranium is particularly susceptible to distant contact results as a result of the structure of this region is significantly weaker and not as efficient in managing the native cranium deformations initiated by distant impression. Common influence factors for producing a basilar skull fracture include the cranium base, facial or mandibular bones, and distant skull impression factors. Fatal basilar cranium fracture can even happen when the torso of a driver or passenger is sufficiently restrained in a vehicular crash however the head is allowed to maneuver on account of the impulsive forces in such a manner that the cervical backbone is distracted from the base of the skull. Robert Hubbard and Jim Downing, was designed specifically to stop this kind of damage. Other comparable restraining systems have been designed to be used in bike racing and equestrian events. It is evident that many of these accidents can occur together, and isolated occurrences of most of these injury, significantly after severe head accidents, are rare. Focal Brain Injury Epidural Hematoma Epidural hematoma can be thought-about a extra complex case of linear cranium fracture.
Buy 500 mg benemid with amex
Second, an applicable diagnostic analysis is important in planning the strategy of therapy pain medication for glaucoma in dogs 500 mg benemid mastercard. Third, the modality of treatment, surgical or endovascular, should maximize efficacy and reduce dangers to the affected person knee pain treatment yoga 500mg benemid visa. Finally, intraoperative monitoring, with neuronal protection during carotid occlusion, may help scale back issues. In every of these pathologies, preservation of the carotid artery is the first goal of both surgical and endovascular treatment. The bigger collection reported mortality charges of 5% to 15% with surgical excision, cerebrovascular complications in 8% to 20% of patients, and postoperative cranial nerve accidents in 32% to 44% of patients. The vascular provide is from the carotid bifurcation, and the first innervation is the carotid sensory branch of the glossopharyngeal nerve. Embryologically, the carotid physique might have constituents of both the third branchial arch mesoderm and neural elements of the neural crest ectoderm. Tumors of these cells have additionally been often known as paragangliomas, glomus tumors, and chemodectomas. Tumors of comparable histology come up in a quantity of places, together with the ciliary body of the orbit, aortic-pulmonary paraganglia, carotid physique (glomus caroticum), middle ear (glomus tympanicum), ganglion nodosum of the vagus nerve (glomus vagale), jugular body (glomus jugulare), and adrenal medulla (pheochromocytoma). Although most glomus tumors seem like composed of nonchromaffin cells which may be physiologically silent, some include secretory granules that will secrete catecholamines just like pheochromocytomas. Anatomic dissection revealed that the construction was contained in a dense meshwork on the base of the carotid bifurcation. Years later, Kohn defined the carotid body as chromaffin cells embedded within the sympathetic nerve fibers in regards to the carotid artery and coined the term paraganglion. The report detailed an aggressive tumor resection with division of the carotid artery; jugular vein; and vagus, hypoglossal, and sympathetic nerves. Most true aneurysms of the cervical carotid artery, nevertheless, are brought on by atherosclerotic disease of the artery. The major objectives of treatment ought to be exclusion of the aneurysm and preservation of adequate cerebral blood circulate. Therefore, the hunterian ligation employed by Cooper for this pathology is now not relevant to most instances. The results of small up to date operative sequence involving preservation of the carotid artery have been good. Painter and coworkers93 reviewed the literature on extracranial carotid aneurysms handled surgically over a 10-year interval by strategies apart from ligation. Of the 61 operative circumstances they found, three patients (5%) had permanent neurological deficits from the surgical procedure, and one died (1. No convincing proof suggests that the illness progresses as a rule, though notable exceptions have been reported. In sufferers with an embolic presentation, antiplatelet treatment similar to aspirin, ticlopidine, or clopidogrel is really helpful. Intervention is warranted in patients whose symptoms persist regardless of antiplatelet remedy. Before dilation, they discovered strain before 25 and 50 mm Hg; after surgical treatment, there were no discernible gradients. Three sufferers died greater than 5 years after the operation from myocardial infarction. With all aneurysms extending to the C1 degree or higher, they have been in a place to revascularize 12 arteries and ligate 3 (one after an extracranial-intracranial bypass). In such circumstances, trapping the diseased section and performing a high-flow vein bypass constitute the preferred treatment. Aneurysms of the highcervical segment may be related to parapharyngeal infection or iatrogenic trauma. In such circumstances, the field is contaminated, and first direct restore of the carotid artery will not be possible. Likewise, endovascular stents will not be indicated because inserting a international physique, corresponding to a stent or stent graft, in an contaminated region may lead to chronic implant an infection. Carotid occlusion is a reasonable different if the patient passes a balloon take a look at occlusion. If the patient fails balloon test occlusion, bypass occlusion with carotid occlusion is the popular long-term strategy. It may be significantly useful in the high cervical area, which is tough to access surgically. Likewise, if the contralateral carotid artery is diseased, preservation of the ipsilateral carotid artery may be preferable to counting on bypass patency. It varieties a false channel or a false lumen that will increase inward to narrow the true lumen or broaden outward to develop a dissecting aneurysm. A pseudoaneurysm might kind when all layers of the arterial wall have been breached. The headache manifested as frontal or periorbital ache in some and as periauricular pain in others. It is but to be established whether males or females are more susceptible to spontaneous carotid artery dissections. However, one research analyzing gender differences in 696 sufferers with spontaneous carotid artery dissections reported a higher incidence in males (n = 399; P <. Women with carotid artery dissections had been youthful and had a higher incidence of multiple dissections. Recent research have shown that dietary status may also be a danger factor for carotid artery dissections. These sufferers have larger plasma ranges of proteases, significantly matrix metalloproteinase 2. In a case-control study using colour duplex sonography, Baumgartner and colleagues108 demonstrated that spontaneous and endothelial-independent (nitroglycerin) vasodilation is impaired in sufferers with spontaneous carotid dissection. Facial sweating is seldom affected, a pattern that reflects the anatomy of the sympathetic fibers. Treatment the mainstay of remedy for sufferers with spontaneous carotid artery dissection is anticoagulant medical remedy. Vertebrobasilar signs come up from interruption of the blood supply to the brain and brainstem. The interruption may be the end result of hypoperfusion brought on by hemodynamic adjustments or by thromboembolic sources. Regional hypoperfusion is the predominant stroke mechanism for patients with posterior circulation ischemia. Large or small vessel occlusive disease happens extra generally in the posterior circulation than thromboembolism. Hemodynamic changes can also end result systemically from cardiac insufficiency or postural hypotension. The pathology that causes hemodynamic adjustments and the sources of emboli often overlap. Emboli or thrombi might originate from vertebral arteries, subclavian artery, aortic arches, pathologic coronary heart valves, abnormal cardiac wall habits, or arrhythmias.
Benemid 500mg buy without prescription
In addition, a choice to stent the carotid or vertebral artery was made if an infarct occurred while the patient was receiving antiplatelet remedy or if a big flow-limiting intimal flap was current pain treatment in lexington ky discount benemid 500 mg online. A traumatic intracranial aneurysm from one of many peripheral branches of the middle cerebral artery is clear breast pain treatment vitamin e purchase 500mg benemid with mastercard. In the sequence of Cohen and colleagues, 1 of 13 patients treated with a naked stent and coiling had a rising intracavernous pseudoaneurysm necessitating occlusion and bypass of the inner carotid artery. In no affected person in this sequence was renewed bleeding seen after a imply follow-up of two. Overall, 21% of patients admitted alive to the emergency department made a good restoration (73 of 349 patients). Only 10 sufferers had been seen on the trauma resuscitation unit of a shock trauma heart alive, 8 of whom underwent surgical procedure and 6 (2. Corkin seen a long-lasting effect on hidden figures test performance when a missile head wound concerned the left hemisphere. The authors reported important drops in intelligence test scores over time in patients with missile head wounds. They postulated the decline in intelligence to be because of the primary effects of the missile head wound and the added results of advancing age and stress on the remaining brain tissue attributable to functioning for decades in a compromised state. There is proof that troopers returning residence from fight duties in Iraq and Afghanistan may endure from poor common well being and be extra vulnerable to cardiovascular complications, each of which can ultimately affect their job efficiency and productiveness. Other systemic effects include cell-mediated immunity, disordered sleep physiology, and symptoms of altered notion. Surgical outcome in 435 patients who sustained missile head wounds during the Iran-Iraq warfare. Penetrating craniocerebral accidents within the Israeli involvement in the Lebanese conflict, 1982-1985. Learning from traditional fight mortality and morbidity knowledge used within the evaluation of combat medical care. Hidden-figures-test performance: lasting results of unilateral penetrating head harm and transient results of bilateral cingulotomy. Penetrating stab wounds to the brain: the timing of angiography in sufferers presenting with the weapon already eliminated. Lebanon, New Hampshire: American Association of Neurological Surgeons; 1999:17-33. Wisconsin Card Sorting Test efficiency based mostly on location and size of neuroanatomical lesion in Vietnam veterans with penetrating head harm. Mild Traumatic Brain Injury in Service Members Returning from Iraq and Afghanistan. Understanding sequelae of harm mechanisms and delicate traumatic brain damage incurred during the conflicts in Iraq and Afghanistan: persistent postconcussive signs and posttraumatic stress disorder. The complexity of the injury, which is usually related to trauma to other organ systems, makes choices about medical or surgical administration important to patient outcome. Gennarelli and coworkers confirmed that the overall mortality is three times higher in trauma sufferers with head harm than in these without intracranial trauma. The severity of the top harm nonetheless stays the strongest predictor of general outcome in multiply traumatized individuals. This pessimism was based on the idea that end result is decided principally by the magnitude of the initial damage and that it incessantly remains poor despite optimal surgical procedure. High-volume lesions (>50 cc) usually bear surgery, whereas small lesions (<25 cc) are often managed with conservative remedy. Once the indications for surgical procedure have been met, early and urgent surgical intervention is suggested to stop further neurological decline, reduce perilesional edema, enhance the native metabolic surroundings, and attenuate evolving ischemic changes. Interestingly, blood constituents were proven to worsen focal ischemia in a study evaluating equal volumes of hematoma with an inert fluid used to generate experimental intracerebral mass lesions. Mass lesions can also alter cerebral metabolism, and their removal has been proven to enhance jugular venous saturation indices. Improvements in early resuscitation, prognosis, neurophysiologic monitoring, and emergency surgical remedy of head injury victims could additionally be reaching a plateau when it comes to additional decreasing mortality and morbidity. Refinements in neurocritical care combined with technologic advancements in diagnostic and monitoring gadgets proceed to supply new avenues for enhancing outcome. At least 25% of patients with mass lesions will clinically deteriorate in the initial 2 to 3 days after damage. Nonsurgical management is detailed within the third version of the "Guidelines for the Management of Severe Traumatic Brain Injury. Management selections in individual patients must take into account a number of factors, corresponding to extracranial accidents, the age of the affected person, preexisting circumstances, and the presence of related intracerebral contusions or hemisphere swelling. In patients with intraparenchymal lesions, corresponding to contusions and intracerebral hematomas, management decisions are more advanced and tough given the risk for coagulopathy and bleeding. Nonoperative administration ought to be considered only if the patient is absolutely aware, the extra-axial mass lesion is the only dominant lesion. The authors utilized the rules of "evidence-based medication" throughout the analysis course of, however the paucity of well-designed, randomized managed trials for surgical lesions prohibited classification of the literature with the "degree of evidence" categories now customary in setting up pointers. Finally, in sufferers who require operative intervention, pressing and fast evacuation of the mass lesion ensures the best end result as a result of ischemic mind damage is dependent on the duration of ischemia. The particular suggestions in the aforementioned doc are introduced within the following sections. Methods Evacuation should be performed by way of craniotomy with or with out bone flap removal and duraplasty. Bifrontal decompressive craniectomy within forty eight hours of harm is a remedy choice for patients with diffuse, medically refractory posttraumatic cerebral edema and resultant intracranial hypertension. Craniotomy with evacuation of the mass lesion is really helpful for patients with focal lesions and the surgical indications listed earlier. Decompressive procedures, including subtemporal decompression, temporal lobectomy, and hemispheric decompressive craniectomy, are remedy options for patients with refractory intracranial hypertension, diffuse parenchymal harm, and scientific and radiographic proof of impending transtentorial herniation. Step 3 (B): Now, also on slice 1, measure the most important diameter orthogonal to A and call this "B" (in centimeters). Step four (C): Count the variety of 10-mm slices that it takes to embody the hematoma. Timing Patients who meet the surgical indications ought to bear pressing operative intervention. Patients with open (compound) cranial fractures depressed greater than the thickness of the skull ought to endure operative intervention to prevent infection. Basal cisterns at the midbrain stage: Compressed or absent basal cisterns are associated with a threefold risk for intracranial hypertension. Primary bone fragment replacement is a surgical choice in the absence of wound an infection on the time of surgery. All administration methods for open (compound) depressed fractures ought to embody antibiotics.
Real Experiences: Customer Reviews on Benemid
Marcus, 51 years: A fast gradient echo, echo planar sequence is used to acquire a quantity of volumes of images through the mind in the course of the first passage of a standard dose of a gadolinium-based contrast agent administered rapidly (5 mL/sec, antecubital vein) as an intravenous bolus through the capillary bed of the brain. Unless urgently addressed, occlusion of the torcular or a dominant transverse or sigmoid sinus will outcome in the fast growth of sustained intracranial hypertension and incessantly demise. Ophthalmic Artery Aneurysms Ophthalmic artery aneurysms come up immediately distal to and in relation to the origin of the ophthalmic artery. In distinction to the dynamic contrastenhanced approach, perfused blood quantity mapping can picture the whole brain volume.
Julio, 25 years: In some sufferers, signs of the syndrome of the trephine may be alleviated by recumbency. However, the distal vertebral artery is easily accessed with a big publicity from the dura to C1 and by eradicating the C1 foramen as inferiorly as the exit of C2. It can be induced by local clot formation or emboli and leads to neuronal injury inside minutes. When the aneurysm lies beneath or proximal to the genu of the corpus callosum, the identical positioning is employed, however the head is prolonged.
Einar, 31 years: Res tl es s Leg Syndrome Founda ti on, Inc, 2001 Medical Bulletin, revi s ed Apri l 2001. A review of the endovascular results alone confirmed a higher fee of full occlusion with smaller aneurysm measurement and anteriorly directed domes. The interval between decompressive surgery and secondary bone flap substitute within the literature varies from four weeks as much as 12 months, throughout which time the unprotected brain is exposed to the risk of harm. Retrolabyrinthine transsigmoid strategy to basilar trunk and vertebrobasilar artery junction aneurysms: technical notice.
Ilja, 38 years: As in any region of the backbone, pseudarthrosis on the cervicothoracic junction is related to tobacco use, previous surgery, and correction of deformity at the involved ranges. If reevaluation after 3 months (6 months after dissection) exhibits persistence of the pathology, oral anticoagulation is stopped, and the patient is kept on antiplatelet therapy for all times. However, there are several techniques that are frequent to all aneurysms, together with patient choice and diagnostic research, anesthetic methods, positioning, neuromonitoring, and brain relaxation that ought to be considered earlier than surgery. If vitality metabolism depends on glucose metabolism, energy failure because of glucose depletion is one other potential explanation for secondary ischemic insults after extreme head harm.
9 of 10 - Review by U. Gelford
Votes: 285 votes
Total customer reviews: 285
