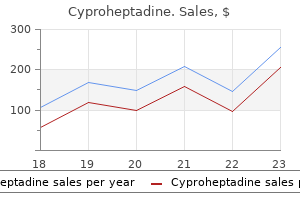
Cyproheptadine dosages: 4 mg
Cyproheptadine packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount cyproheptadine 4 mg amex
Proceedings of the 16th International Congress on Acoustics and one hundred and thirty fifth Meeting of the Acoustical Society of America; 1998 allergy testing louisville ky cheap cyproheptadine 4 mg with amex. Early observations of the impact of extracorporeal shockwave lithotripsy on blood stress: a prospective randomized control scientific trial allergy treatment los angeles cyproheptadine 4 mg on line. A decrease in blood strain after pyelolithotomy however not extracorporeal lithotripsy. Apatite plaque particles in inside medulla of kidneys of calcium oxalate stone formers: osteopontin localization. Renal harm during shock wave lithotripsy is significantly reduced by slowing the speed of shock wave delivery. Upper and mid-ureteric stones: a prospective unrandomized comparability of retroperitoneoscopic and open ureterolithotomy. Renal capsular block: a novel technique for performing percutaneous nephrolithotomy under native anesthesia. The clinical analysis office of the endourological society percutaneous nephrolithotomy international study: indications, problems and outcomes in 5803 patients. The clinical research workplace of the endourological society ureteroscopy international examine: indications, problems, and outcomes in eleven,885 sufferers. Minimal static excess stress minimises the effect of extracorporeal shock waves on cells and reduces it on gallstones. Biological results of shock waves: kidney haemorrhage by shock waves in dogs�administration rate dependence. Shock wave lithotripsy causes ipsilateral renal harm distant from the focus: the role of regional vasoconstriction. A novel strategy of ultra-mini-percutaneous nephrolithotomy: introduction and an initial expertise for therapy of higher urinary calculi lower than 2 cm. New techniques of ultrasound and color Doppler in the prospective evaluation of acute renal obstruction: do they exchange the intravenous urogram A multivariate evaluation of risk elements associated with subcapsular hematoma formation following electromagnetic shock wave lithotripsy. Report of the United States cooperative examine of extracorporeal shock wave lithotripsy. Operator expertise and enough anesthesia improve remedy consequence with third-generation lithotripters. Flexible ureterorenoscopy and holmium laser lithotripsy for the administration of renal stone burdens that measure 2 to 3 cm: a multi-institutional expertise. New onset hypertension after extracorporeal shock wave lithotripsy: age associated incidence and prediction by intrarenal resistive index. Percutaneous nephrolithotomy in horseshoe kidneys: applied anatomy and medical experience. Combined percutaneous and extracorporeal shock wave lithotripsy for staghorn calculi: an alternative to anatrophic nephrolithotomy. Spinal-epidural anesthesia versus common anesthesia within the management of percutaneous nephrolithotripsy. Is routine radiological surveillance necessary after uncomplicated ureteroscopic stone removal Electrokinetic lithotripsy: security, efficacy and limitations of a brand new type of ballistic lithotripsy. Success and short-term complication charges of percutaneous nephrostomy throughout being pregnant. Percutaneous nephrolithotomy for caliceal diverticular calculi: a novel single stage approach. A double-blind randomized controlled trial of steady intravenous Ketorolac vs. Optimising an escalating shockwave amplitude remedy technique to defend the kidney from damage throughout shockwave lithotripsy. Focused ultrasound to expel calculi from the kidney: safety and efficacy of a scientific prototype device. An algorithm for analysis and remedy of management and problems of urolithiasis throughout being pregnant. Percutaneous renal and ureteric stone extraction: report on the primary 500 operations. Comparison of one hundred fifty simultaneous bilateral and 300 unilateral percutaneous nephrolithotomies. A study of resistive indices within the arcuate arteries of the kidney over the course of gestation. Urinary excretion of calcium in late pregnancy and its relation to creatinine clearance. Cost effectiveness of electrohydraulic lithotripsy v Candela pulsed-dye laser in administration of the distal ureteral stone. Extracorporeal shock wave lithotripsy: development, instrumentation, and current standing. Blood stress changes following extracorporeal shock wave lithotripsy and other forms of therapy for nephrolithiasis. Computed tomography-determined stone-free charges for ureteroscopy of upper-tract stones. Shock wave lithotripsy not related to growth of diabetes mellitus at 6 years of follow-up. Percutaneous nephrolithotomy use is growing within the United States: an evaluation of developments and issues. Comparison of intravenous sedativeanalgesic strategies for outpatient immersion lithotripsy. Randomized managed, multicentre scientific trial evaluating a dual-probe ultrasonic lithotrite with a single-probe lithotrite for percutaneous nephrolithotomy. Long term results of shock wave lithotripsy for nephrolithiasis: a nineteen 12 months research. A randomized scientific trial of ureteroscopy and percutaneous nephrolithotomy for lower pole stones between 11 and 25 mm. Clinical utility of extracorporeal shock wave lithotripsy utilizing microexplosions. Size and location of defects on the coupling interface have an effect on lithotripter performance. Percutaneous nephrolithotomy under native infiltration anesthesia: a single-center expertise of 2000 Chinese circumstances. Does a smaller tract in percutaneous nephrolithotomy contribute to much less invasiveness Efficiency and efficacy of different intracorporeal ultrasonic lithotripsy items on an artificial stone mannequin. Predictive value of urinary cultures in assessment of microbial colonization of ureteral stents. Outcomes of latest percutaneous nephrostolithotomy in morbidly overweight sufferers. The outcomes of ureteral stenting after ureteroscopic lithotripsy for ureteral calculi: a scientific evaluation and metaanalysis. Extracorporeal shock wave lithotripsy for renal stone disease: technical and clinical aspects. Ureteral and bladder lesions after ballistic, ultrasonic, electrohydraulic, or laser lithotripsy.
4 mg cyproheptadine fast delivery
Therefore the approach to a patient with true hyponatremia begins with an assessment of volume status allergy symptoms penicillin buy cyproheptadine 4 mg with visa. Clinical features such as skin turgor allergy pills buy cyproheptadine 4 mg cheap, orthostatic hypotension, jugular venous distension, ascites, and respiratory crackles can all be useful in this decision. If the hyponatremic affected person is hypervolemic, whole body sodium can be low, normal, or excessive. Demeclocycline, in doses ranging from 600 to 1200 mg/day, induces vasopressin-resistant diabetes insipidus that corrects the serum sodium within 1 to 2 weeks (Goh, 2004). Therapy of hyponatremia is directed each at the trigger of the condition and the water imbalance itself. Patients with acute extreme hyponatremia symptomatic with confusion, convulsions, or coma ought to bear fluid restriction plus the administration of hypertonic (3%) saline (about 1 mL/kg/hr). Fluid overload is unlikely as long as fluid intake is restricted, but fluid may be further decreased by simultaneous administration of a loop diuretic corresponding to furosemide, which causes excretion of hypotonic fluid equal to half-normal saline. The serum sodium focus should be raised to no extra than 25 mEq/L in the first 48 hours, at a rate of not more than 2 mEq/L per hour, and the goal objective ought to be a hundred and twenty to one hundred twenty five mEq/L. Total sodium deficit to reach this level could be calculated as (Volume of distribution) � physique weight (kg) � (125 - plasma [Na]) where volume of distribution is 0. During acute intervention for extreme hyponatremia, frequent electrolyte measurements and affected person reassessment are required. At that point, water restriction and reversal of underlying causes ought to suffice. Obviously, sufferers with associated hypovolemia ought to have this corrected with the appropriate quantity of normal saline. Hypernatremia the underlying drawback of hypernatremia is a disorder of urine concentration with insufficient water intake (Adrogue and Madias, 2000). Symptoms are nonspecific and overlap with those seen in hyponatremia, with the early incidence of restlessness, nausea, and vomiting, which can progress to tremor, lethargy, and coma. Indeed, mortality is higher with hypernatremia than with most other electrolyte issues. Most patients with an intact thirst mechanism and free access to water can forestall hypernatremia and, as such, the situation is extra common on the extremes of age. Again, the method to a affected person with hypernatremia begins with an assessment of fluid status. Hypovolemia is frequent and could additionally be because of renal situations that fail to adequately focus the urine (loop diuretics, postobstructive diuresis), or to circumstances of extrarenal water loss, such as seen with burns, diarrhea, or fistulae. Patients with hypervolemia could have a metabolic or iatrogenic reason for prime sodium in excess of the elevated whole body water. In neurogenic diabetes insipidus, vasopressin deficiency is mostly caused by destruction of the neurohypophysis. To produce symptomatic polyuria, 80% to 90% of the neurosecretory neurons must be destroyed at or above the level of the infundibulum. Because of the lowered vasopressin stage, the kidney excretes a excessive quantity of dilute urine. This leads to a reduction in total body water, an increase in total body osmolality, and thus hypernatremia. Compensatory water intake decreases plasma osmolality (and Na+ concentration) toward normal, however they stabilize on the threshold stage for thirst, which is barely above regular. As in all forms of diabetes insipidus, the power of the kidney to maximally concentrate the urine in response to vasopressin is also impaired in neurogenic diabetes insipidus. This abnormality happens as a outcome of the medullary osmotic gradient is decreased by the excessive urine circulate. In nephrogenic diabetes insipidus, secretion of vasopressin by the neurohypophysis is normal, however renal responsiveness to the hormone is attenuated or absent, and urinary concentrating ability is impaired (Sasaki, 2004). Several different mutations of the aquaporin gene have been identified, which contribute to the pathogenesis of this dysfunction (Leung et al, 2005). Therapy of hypernatremia is directed at fluid deficit, water replacement, and reversal of underlying causes. If the affected person is awake and never symptomatic, oral hydration with water is adequate. The water deficit can be calculated as (Volume of distribution) � body weight (kg) � (plasma [Na]/140 - 1)) the place, once more, quantity of distribution is zero. For patients with central diabetes insipidus, desmopressin (a artificial exogenous vasopressin) could be administered intranasally. For nephrogenic diabetes insipidus, the underlying cause (lithium, hypercalcemia) must be treated. Urinary excretion may be elevated in the kidney via elevated aldosterone, a excessive sodium load in the distal tubule, and by acidosis. The commonest iatrogenic causes are diuretics, laxatives, amphotericin, theophylline, and postobstructive diuresis. Metabolic causes embrace circumstances associated with elevated aldosterone, such as adrenal adenoma, Cushing syndrome, and adrenal carcinoma. Therapy is directed toward correction of the underlying trigger and oral or parenteral potassium supplementation. Hyperkalemia Hyperkalemia usually reflects decreased renal excretion of potassium or a shift out of cells into the extracellular house (usually by acidosis). Therapy to enhance intracellular potassium must be coupled with a therapy to take away potassium shops, or the hyperkalemia will recur after infusions cease. Potassium-binding change resins (kayexalate, calcium resonium) can be utilized for this purpose orally or by enema. Finally, hemodialysis can most rapidly and utterly remove extracellular potassium. Because neuromuscular excitability is carefully linked to serum potassium ranges, extremes of low or high values can result in cardiac arrhythmias and demise. Furthermore, pH determines the web cost of proteins, which influences protein conformation and enzyme-binding traits. There is a big production of acid by the metabolism of carbohydrates and fat, largely within the form of carbon dioxide, at roughly 15,000 mmol per day. The catabolism of ingested proteins to amino acids is one other source of acid manufacturing, estimated at between 50 and 100 mEq of H+ per day (sulfate from the three sulfur-containing amino acids; phosphate from phosphoproteins). A buffer is just a mix of a weak acid and its conjugate base, or a weak base and its conjugate acid, that resists changes in pH when one other acid or base is added. Within the cell, proteins and phosphates, that are present in greater concentrations than in the blood, turn into essential as properly. Changes in pH are ruled by the HendersonHasselbalch equation, which usually is pH = pKa + log base/acid When specifically formulated for the bicarbonate system it turns into pH = 6.
Diseases
- Hydronephrosis peculiar facial expression
- Mucolipidosis type 4
- Central serous chorioretinopathy
- Syndactyly type 3
- Cryptorchidism arachnodactyly mental retardation
- Pfeiffer Palm Teller syndrome
- Gliomatosis cerebri
- Dimitri Sturge Weber syndrome
- Alveolar soft part sarcoma
- Lymphedema hereditary type 1
Cyproheptadine 4 mg order line
Patients can be screened for thrombophilia by checking clotting components allergy forecast chicago mold 4 mg cyproheptadine effective, together with the platelet rely allergy shots migraines cheap 4 mg cyproheptadine free shipping, prothrombin time, partial thromboplastin time, and activated protein C resistance ratio (factor V Leiden mutation). The particulars of previous abdominal or pelvic surgical procedure might have a significant influence on the optimum placement of a renal allograft. The bodily examination should embrace descriptions of scars, catheters, and stomas. Additional urologic research could additionally be indicated to evaluate the anatomy of the urinary tract, bladder function, and risk for malignancy (Table 47-1). In patients on peritoneal dialysis, fluid in the pelvis could be misinterpreted as residual urine. If patients have an inflatable penile prosthesis with an abdominal reservoir, it can be mistaken for the urinary bladder or make exposure of the bladder more difficult. It additionally may enhance the administration of hypertension and reduce the risk for cardiac issues (Shemin et al, 2001). Therefore the indication for native nephrectomy must be balanced by the risk of observation. Some surgeons prefer to do the nephrectomy on the time of transplant, however this may increase the chance for problems with the transplant kidney. Patients who might undergo transplantation before the start of dialysis may profit from post-transplant nephrectomy. Asymptomatic patients with severely enlarged kidneys might require native nephrectomy to make room for the renal allograft. Adequate space in the iliac fossa can typically be assessed by a mixture of physical examination and stomach imaging. Nephrectomy can be performed concurrently with the renal transplant, but this will improve perioperative complications and morbidity (Fuller et al, 2005). In some circumstances a much less selective -blocker additionally will be useful within the therapy of hypertension. Caution is suggested in performing transurethral resection in anuric patients due to the excessive risk for bladder neck contracture or prostatic fossa strictures. Coma as evidenced by no eye opening and no response to ache aside from spinal cord reflexes B. Disconnect ventilator and place large-bore catheter down the endotracheal tube to deliver one hundred pc O2 or place on continuous positive airway strain with one hundred pc O2 C. Confirmatory tests (electroencephalogram, cerebral angiography, nuclear medication brain scan) A. May shorten the period of statement, particularly in kids and young adults C. Ideally the urinary reservoir ought to have a capacity of at least 200 mL, low storage strain, an antirefluxing ureteral anastomosis, and the power to empty utterly. Patients with extended anuria could lose bladder capacity, but even small defunctionalized bladders will incessantly regain normal volume inside weeks of transplantation (Wu et al, 2008). Lower urinary tract reconstruction is best accomplished with adequate urine production to reduce the chance for stricture, stones, infection, and lack of compliance. The recipient is inspired to deliver potential residing kidney donors to academic seminars. Renal transplant outcomes are considerably improved with a residing in comparison with a deceased donor. The final pairing of a kidney donor with a recipient is a fancy process that includes both immunologic and nonimmunologic elements. The Act referred to as for the community to be operated by a non-public, nonprofit group under federal contract. Organ procurement personnel screen all eligible donors and assign a workers member to discuss organ donation with the following of kin. Neurologic standards for brain dying include coma, irreversibility, known mind harm, and absence of mind stem reflexes (Box 47-2). In this example, a person or family may consent for donation only when demise is decided by cessation of cardiopulmonary operate. When the choice to withdraw care is made, ventilator help is discontinued in the intensive care unit or operating room. Death is said by absence of spontaneous respiration and sustained asystole for five minutes before organ recovery begins. To optimize the recovery of both thoracic and abdominal organs, a median sternotomy and midline incision are used for extensive publicity. Cannulas for the administration of preservation answer are inserted into the aorta, clamps are applied, venous effluent is vented, and the organs are flushed, instantly cooled with ice chilly saline slush, carefully separated, inspected, and packaged for transportation. Spleen and lymph nodes are eliminated for histocompatibility testing, and iliac vessels are removed for vascular reconstruction of pancreas and liver grafts. Chapter47 RenalTransplantation 1075 time, and cut back the need for dialysis after transplant (Opelz and D�hler, 2007). In common, each the warm and chilly ischemia times ought to be minimized to promote restoration of the allograft. Allocation the variety of patients listed for kidney transplantation continues to expand disproportionately to the number of kidney transplantations performed annually. The inadequate supply of deceased-donor kidneys is one of the factors that have elevated the use of "marginal" deceaseddonor organs and the variety of living donor kidneys in the past decade. Multiorgan transplant recipients, pediatric candidates, and former residing kidney donors obtain precedence. For most kidney transplant candidates, nonetheless, the most important think about receiving an organ provide is time spent on the waiting record. The class of donor organs any recipient is prepared to settle for should be determined by the patient and transplant doctor. Depending on size, pediatric donor kidneys could additionally be transplanted en bloc, or, if giant sufficient, cut up and allotted to two recipients. Recipients of pediatric donor kidneys ought to ideally be lower than eighty kg, and some programs prefer not to use small kidneys in highly sensitized patients, however methods vary throughout programs. A KidneyPreservation the renal tubular sodium-potassium pump is required to maintain a high intracellular focus of potassium. Cellular swelling reduces perfusion, which finally ends up in delayed operate of the allograft and increased immunogenicity. Hypothermia (4� C) reduces cellular power necessities and preservation solutions are designed to maintain intracellular electrolyte composition (Table 47-2). Simple chilly storage is inexpensive and facilitates the transportation of the donor kidney. The Centers for Disease Control and Prevention reviewed the danger for transmission of viral diseases with organ transplantation (Centers for Disease Control and Prevention, 1994). It is essential to note that each one donor organs, even these not thought of larger risk by the Centers for Disease Control and Prevention, have the potential to transmit illness.
Order cyproheptadine 4 mg without a prescription
LaboratoryStudies the initial workup of a affected person suspected of getting urinary tract obstruction should begin with a urinalysis and microscopic analysis allergy medicine pink pill purchase 4 mg cyproheptadine with visa. Urinalysis the urinalysis and microscopic analysis is necessary in the complete analysis of a patient suspected of having urinary tract obstruction and/or renal failure allergy forecast fort wayne generic 4 mg cyproheptadine with visa. Creatinine remains imprecise, nonetheless, due to variability with age, gender, race, and relationship with muscle mass. A evaluation of the imaging modalities presently obtainable and their advantages and limitations is offered within the following part. Ultrasonography Renal ultrasonography remains a first-line imaging modality in the analysis of a affected person suspected of having urinary tract obstruction due to its availability, low price, and lack of ionizing radiation. The renal ultrasound primarily provides anatomic details about the kidney, including renal measurement, cortical thickness, corticomedullary differentiation, and grade of collecting system dilation. Parenchymal thinning and small renal measurement can be proof of continual renal obstruction, and bladder distention in affiliation with hydronephrosis could be suggestive of bladder outlet obstruction. The introduction of duplex Doppler sonography was subsequently suggested as a means to enhance the power of ultrasonography to diagnose renal obstruction in patients. It has been proven that after a brief period of prostaglandin-mediated vasodilation, renal blood move decreases and renal vascular resistance increases in response to obstruction. Color Doppler ultrasonography has been shown to reliably identify ureteric jet dynamics within the bladder, and this has advanced as one other diagnostic tool to distinguish obstructive from nonobstructive hydronephrosis. Burge and colleagues (1991) demonstrated that there was a significant decrease within the frequency of ureteral jets in patients with obstructing ureteral stones in comparison with the normal ureter. Although the evaluation of ureteral jets is definitely utilized throughout routine ultrasonography and may supply some valuable perception into the presence of obstruction, it does require good hydration of the patient and is proscribed by the requirement of a traditional contralateral accumulating system for comparability. One of the most common causes of urinary tract obstruction is the presence of renal or ureteral calculi. Direct visualization of stones can be troublesome on ultrasound, due to the presence of overlying bowel fuel and the relative depth of the ureter inside the pelvis, and could be further sophisticated in obese sufferers with massive amounts of intervening fats (Cheng et al, 2012). Because of those limitations, ultrasound is primarily used as a first-line investigative tool solely in pediatric and pregnant sufferers, but it may be used for routine follow-up in all sufferers with urolithiasis. It is necessary to remember that measurement of differential renal function and tracer washout will differ relying on the protocol and radiopharmaceutical used, and care should be taken when deciphering outcomes if comparative research have been carried out utilizing different protocols or radiopharmaceuticals. The initial phase is characterized by speedy uptake of the radiopharmaceutical by the kidneys, reflecting renal perfusion. Urinary obstruction can diminish the rate of uptake of the radiotracer in the course of the second phase and might therefore alter the evaluation of differential renal operate. The third part is the excretory part and is characterised by a gradual decrease in renal counts over time. The third part is usually augmented by the administration of a diuretic (diuretic renogram) to induce excessive urine circulate and prevent the false constructive outcomes that can be attributable to urine stasis in a dilated amassing system. By convention, a kidney is considered unobstructed if the time for half of the tracer to leave the amassing system (T1/2) is lower than 10 minutes, is equivocal if the T1/2 is 10 to 20 minutes, and is taken into account obstructed if the T1/2 is greater than 20 minutes. Falsepositive outcomes can be seen in the presence of dehydration because of the suboptimal response to a diuretic agent, poor renal operate, high-grade reflux, and within the presence of massive collecting system dilation with urinary stasis (Goldfarb et al, 2006). Renal immaturity in neonates additionally could generate false-positive outcomes (Karam et al, 2003). To enhance the accuracy of diuretic renography and restrict falsepositive outcomes, patients ought to be well hydrated for the study. Bladder distention and elevated bladder pressures can limit the ability of the upper urinary tract to drain and will artificially prolong the excretory part of the examine. Patient place through the research also appears to affect results, and urine circulate may be slow and resemble obstruction when the patient is supine. Timing of diuretic administration is somewhat controversial, and multiple different protocols have been established. Traditionally, furosemide is injected 20 minutes after the radiopharmaceutical is administered (F+20), although the diuretic could be administered quarter-hour before tracer injection (F-15) or on the time of tracer injection (F+0). The advantages of the F+20 approach are that the modifications to the drainage curve caused by furosemide may be noticed, and if sufficient kidney washout has occurred during the fundamental renogram, one can probably avoid the administration of furosemide (Piepsz, 2011). With earlier administration of furosemide (F-15, F+0), urine flow is elevated dramatically throughout the entire study, and Turkolmez and colleagues (2004) discovered that these protocols allowed clarification of obstruction in circumstances of equivocal F+20 studies. The disadvantage of the F+0 protocol is that early furosemide injection can lead to acceleration of renal transit and an underestimation of renal function on the aspect with a short transit time (Donoso et al, 2003). An unenhanced section is initially performed, followed by a nephrogenic phase obtained approximately one hundred to one hundred twenty seconds after contrast injection, and an excretory section is carried out after a greater time delay to evaluate the urothelium. In addition to stones, calyceal diverticulum, crossing vessels inflicting ureteropelvic junction obstruction, duplication anomalies in nonfunctioning techniques, ureteroceles, and ectopic ureteral insertions can all be visualized with good accuracy. Because of these dangers, low-dose protocols have emerged with very little loss in diagnostic accuracy (Poletti et al, 2007). Stones smaller than three mm, impaction on the ureterovesical junction, and patient weight problems, nevertheless, have been shown to impair the diagnostic accuracy of low-dose strategies (Kennish et al, 2010). Renal scintigraphy can give false-positive results in the face of huge collecting system dilation or poor renal perform, as a end result of continued filling, somewhat than drainage, of the accumulating system happens in response to furosemide, resulting in an obvious prolongation within the calculated washout time. The Whitaker check entails placement of a percutaneous needle within the accumulating system of the kidney and the infusion of distinction at a rate of 10 mL/min. A urodynamic catheter can also be positioned within the bladder, and intravesical pressures are monitored and subtracted from measured intrapelvic pressures through the infusion. Intrapelvic pressures are noted at the time that distinction is first seen extending past the ureteropelvic junction and past the ureterovesical junction. Pressures lower than 15 cm H2O are thought of normal, higher than 22 cm H2O are indicative of obstruction, and between 15 and 22 cm H2O are considered indeterminate. Although the reproducibility and clinical utility of the Whitaker take a look at have been questioned (Djurhuus et al, 1985), the test lately has been shown to decide or contribute to therapeutic management in 84% of instances of suspected obstruction and to accurately predict both obstruction and nonobstruction in 77% of circumstances (Lupton and George, 2010). A examine by Veenboer and de Jong in 2011 demonstrated a 100 percent unfavorable predictive worth in the capacity of the Whitaker test to diagnose the absence of obstruction. Although the Whitaker test has restricted applicability in scientific follow, it continues to have a valuable function in the evaluation of equivocal higher urinary tract obstruction, especially when noninvasive investigations are inconclusive. The incidence of nephrogenic systemic fibrosis in patients with threat elements has been demonstrated to be 3%, and new recommendations now limit the utilization of gadolinium in patients with renal impairment (Cerwinka and Kirsch, 2010). Retrograde Pyelography Retrograde pyelography refers to the injection of distinction into the higher amassing system through a cystoscopic strategy. The approach accurately defines ureteral and higher collecting system anatomy and might determine the situation of an obstructive lesion. It is most often used to define the anatomy of the accumulating system when it has not been adequately defined by different imaging modalities or when a patient has risk factors for receiving iodinated distinction material. Because retrograde pyelography involves intubation of the ureter with a catheter, micro organism may be introduced into the upper urinary tract in the course of the procedure. Excretory Urography Excretory urography was beforehand thought-about the imaging modality of choice in the analysis of sufferers suspected of having urolithiasis and/or urinary tract obstruction.
Buy cyproheptadine 4 mg with mastercard
Fascial interposition has been found to decrease vasectomy recanalization rates essentially the most significantly allergy report austin cyproheptadine 4 mg generic line. Several trials have been carried out utilizing irrigation of the stomach ends of the vas deferens with saline allergy symptoms shortness of breath generic cyproheptadine 4 mg overnight delivery, but there was no distinction in time to azoospermia (Cook et al, 2007b). Open-ended vasectomy, by which the testicular portion of the vas deferens stays patent, is another method that has been evaluated with the goal of reducing epididymal stress by performing intraluminal cautery or another methodology of occlusion on the stomach finish, whereas leaving the testicular finish unoccluded. The granulomas are thought to scale back pressureinduced damage to the epididymis, however they increase the vasectomy failure price to 7% to 50% (Shapiro and Silber, 1979; Goldstein, 1983). There is a major lower within the failure rate with open-ended vasectomy when fascial interposition is carried out (decreasing the failure price by approximately 7%) (Li et al, 1994). One procedural side is that excising a prolonged (>1 cm) section of vas deferens is related to the need for a better scrotal incision, probably up to the decrease inguinal region, with the potential for anastomotic pressure with microscopic vasectomy reversal. Vasectomy reversal can be far harder when a lengthy portion of the vas deferens has been excised, with concomitant increases in operative time, size of incision, and postoperative pain (Practice Committee of the American Society for Reproductive Medicine, 2006). Another procedural aspect is the location alongside the length of the vas deferens where the vasectomy is carried out. Experts in microsurgery agree that the anastomosis is least problematic when the lumen of the vas deferens is largest and most concentric, versus the lumen within the epididymis or the convoluted vas (Mammen et al, 2008). Prospective research present that the size of the testicular vas deferens present at the time of reversal has a direct correlation with the presence of seminal fluid containing intact sperm at the time of microscopic vasectomy reversal. For every 1-cm improve in testicular remnant size, the likelihood of entire sperm being present increases fourfold (Witt et al, 1994). Division of the vas deferens ought to be performed approximately three cm distal to the cauda of the epididymis in the straight portion of the vas deferens on the time of vasectomy. All occlusive modalities for vasectomy carry a equally high efficacy by means of postprocedure azoospermia. To date, no particular studies on occlusion approach as a predictor of reversal success have been carried out. Lowvoltage thermal occlusion with intraluminal electrocautery within the belly and testicular ends of the divided vas deferens reduces recanalization rates to less than 0. Vasectomy failure charges have been reported to be lower than 1% when the testicular and belly ends of the divided vas deferens are occluded with hemoclips (Moss, 1974; Bennett, 1976). Interposition of dartos fascia between the divided ends of the vas deferens is another technique for occlusion. This methodology has been reported to scale back the recanalization price even additional, to practically zero (Esho and Cass, 1978; Sokal et al, 2004). One is that dilation of the epididymal duct with obstruction of the testicular finish of the vas deferens produces interstitial fibrosis. Another theory is that extravasation of spermatozoa, with epididymal duct rupture forming a sperm granuloma at the site the place the vas deferens is transected, ends in perineural fibrosis and irritation because sperm are highly antigenic (McMahon et al, 1992). This theory contradicts the previous perception that sperm granulomas are protecting against postvasectomy pain syndrome by relieving strain, though most sperm granulomas are asymptomatic (Tandon and Sabanegh, 2008). It is unclear why some sufferers develop long-term signs and others develop transient signs. Conservative remedy must be the first-line remedy and consists of scrotal elevation and support, warmth or ice (as needed for comfort), and nonsteroidal anti-inflammatory drugs. Conservative therapy should be employed for at least three months for postvasectomy pain. Spermatic twine blocks and pain administration methods ought to be considered after failure of conservative remedy. Surgical therapy may be considered on an individualized foundation if the aforementioned strategies fail. When pain is clearly localized to a sperm granuloma, excision of the granuloma and intraluminal cautery occlusion of the vas deferens could relieve the ache and stop recurrence (Schmidt, 1979). Epididymectomy has been performed in patients who had level tenderness to the epididymis and epididymal dilation after vasectomy and failed conservative remedy. Predictors of poor outcomes with epididymectomy are atypical symptoms, concomitant erectile dysfunction, and a normal-appearing epididymis on scrotal ultrasonography (West et al, 2000). Of patients who have been properly selected for epididymectomy, 50% have been cured of postvasectomy ache syndrome (Chen and Ball, 1991). The patient must think about that vasectomy reversal will not be possible after epididymectomy. Vasectomy reversal rendered 69% of patients with postvasectomy pain syndrome pain-free (Nangia et al, 2000). Although it has been evaluated in solely a small variety of sufferers, microscopic denervation of the spermatic twine in patients who failed conservative therapy resulted in full ache reduction in 76% of these males (Ahmed et al, 1997). The final resort consideration after failure of conservative and more invasive interventions have failed is orchiectomy for severe intractable pain after vasectomy. Pain reduction was reported in 73% of men who underwent inguinal orchiectomy versus 55% of men who underwent scrotal orchiectomy for postvasectomy ache syndrome (Davis et al, 1990). Minimizing irritation near the vas deferens would provide the optimum situation for microscopic vasectomy reversal in the future (Mammen et al, 2008). Time to reach azoospermia is variable, though greater than 80% of sufferers achieve azoospermia by 3 months and after 20 ejaculations. These information point to obtaining a semen evaluation at 3 months and 20 ejaculations after vasectomy to reveal azoospermia. Additional samples ought to be submitted if the preliminary semen evaluation has motile sperm or higher than 100,000 nonmotile sperm/mL. Vasectomy must be repeated if any motile sperm are seen within the ejaculate 6 months after the preliminary vasectomy (American Urological Association, 2012). This take a look at was developed to enhance compliance with postvasectomy evaluation of semen parameters. The SpermCheck Vasectomy check was 96% correct at predicting whether sperm counts had been larger or lower than a threshold of 250,000 sperm/ mL (Klotz et al, 2008). Local complications of vasectomy include hematoma, infection, Fournier gangrene, chronic scrotal ache, and traumatic fistula/scrotal sinus (Awsare et al, 2005). The most essential predictor of postoperative complications is surgeon quantity and experience (Kendrick et al, 1987). The rate of an infection from vasectomy with the standard approach was reported to be between 12% and 38% but decreased to 0. Although exceedingly uncommon, Fournier gangrene has been reported as a complication in males present process vasectomy (de Diego Rodr�guez et al, 2000; Romero P�rez et al, 2004). The medical literature on postvasectomy ache syndrome, or long-term scrotal pain after surgery, consists of research with small pattern sizes, nonvalidated pain measures, excessive nonresponse rates, and variable consequence measures. The most robust study identified the incidence of continual scrotal ache extreme enough to search medical consideration to be zero. Detection bias is assumed to be the supply of this association of prostate most cancers with vasectomy (Millard, 1999). Previous studies advised that vasectomy may be a danger issue for sufferers with main progressive aphasia, a dementia syndrome with aphasia because the presenting symptom (Weintraub et al, 2006). Of males who endure vasectomy, 60% to 80% have detectable levels of antisperm antibodies in the serum (Fuchs and Alexander, 1983).
Syndromes
- Balancing your time between activity, rest, and sleep
- The cause of the osteonecrosis
- Problems urinating, incontinence (leaking urine), feeling of incomplete bladder emptying, difficulty beginning to urinate
- Renal duplex ultrasound examines the kidneys and their blood vessels.
- Vomiting
- Put a loop of fish line through the bend of the fishhook so that a quick jerk can be applied and the hook can be pulled out directly in line with the shaft of the hook.
Cyproheptadine 4 mg purchase otc
More just lately allergy jokes 4 mg cyproheptadine cheap with visa, Iqbal and colleagues (2013) reviewed their expertise with struvite stones allergy medicine jittery discount cyproheptadine 4 mg free shipping. They reported that 60% of pure struvite�stone formers and 77% of combined struvite�stone formers had metabolic abnormalities on 24-hour urine collections. Cystinuria Cystinuria is attributable to an autosomal recessive error of transepithelial transport involving the intestine and kidneys (Thier et al, 1965; Pak and Fuller, 1983). In this illness, sufferers are unable to reabsorb the dibasic amino acids: cystine, ornithine, lysine, and arginine. The resultant accumulation of cystine causes crystallization when concentrations rise above the saturation point (~250 mg cystine per liter of urine) (Pak and Fuller, 1983). Patients with this dysfunction may present at a younger age and should have affected first-degree family members. The stones are often yellow and waxy and are relatively faint on plain radiography. Historically, a diagnosis of cystinuria was made with the use of a sodium nitroprusside spot test that turned purple in the presence of cystine (Smith, 1977). Although this check is a useful screening adjunct, quantitative measurements of cystine may be difficult to carry out due to interference from other sulfhydryl-containing compounds (such as medications used to treat this disorder) or from vital variances with minor changes in urine pH or creatinine content (Pak and Fuller, 1983). Coe and colleagues (2001) developed a more reliable methodology of cystine supersaturation measurement that will significantly assist in the analysis and particularly the management of cystinuria (Nakagawa et al, 2000). Patients with cystinuria could demonstrate further metabolic anomalies on 24-hour urine research (Sakhaee et al, 1989). In controlled dietary evaluation of 27 patients with cystinuria, hypercalciuria was noted in 18. A focused social history ought to elucidate these components and permit for proper identification and subsequent counseling. Plain movie of a affected person with bilateral staghorn calculi composedentirelyofstruvite. NoDisturbances Pak and associates (1980a) estimated that 3% of all sufferers present process a full metabolic evaluation will show no abnormalities. Furthermore, it is very important do not overlook that a 24-hour urine collection represents a pooled sample. Heavy oxalate loading at one specific meal or bolus replacement of fluids at the finish of a piece day may produce common values that look normal, but truly hide periods of maximum urine parameters that promote stone formation. It is very possible (and fairly likely) LowUrineVolumes(<2000mL) Some patients will exhibit only a few abnormalities other than low urine volumes on a whole evaluation. From a simplistic view, a low quantity of urine output will focus the molecular elements of crystal formation and raise the supersaturation risk. Intuitively, a patient with a relative state of dehydration will development toward acidic urine, decreasing the urine pH towards the pKa of uric acid (5. Many patients with low urine volumes work in professions that induce high insensible losses of fluid. Calcium load samples have been obtained over a 4-hour interval subsequent to oral ingestion of 1 g calcium. The diagnostic criteria for the 12 principal classifications described on this part are summarized in Table 52-7. Unfortunately, it can be tough to reach consensus concerning particular details from the out there literature. In this amalgam of college and private apply sufferers, the average improve in urinary quantity was only zero. In addition, intermittent compliance may not be effective, because small, early stones may develop during times of intense dehydration. At least one creator suggested that if a affected person is ready to voluntarily pressure fluid consumption long enough to dilute renal concentrating skills, then thirst mechanisms will take over and help maintain a excessive fluid consumption and excessive urine output (Burns and Finlayson, 1981). Unfortunately, the newer data from Parks and colleagues (2003a) has not proved this finding to be dependable. Water Hardness If water consumption is so important, is there a distinction between ranges of water hardness that might ameliorate or increase its benefit This concept has been the subject of conflicting articles inside the common urologic and epidemiologic literature. In one study, sufferers with a identified historical past of calcium nephrolithiasis have been divided in accordance with postal zip codes. Twenty-four-hour urine measurements have been compared, as was the historical past of stone episodes (Schwartz et al, 2002). Although the 24-hour urine calcium, magnesium, and citrate levels elevated instantly with consuming water hardness, no significant change was found in urinary oxalate, uric acid, pH, or volume. Most importantly, the number of whole lifetime stone episodes was comparable between sufferers residing in areas with delicate public water and exhausting public water. The authors famous that though water hardness can alter urinary parameters, this issue finally seems to have little effect on scientific outcome. These findings are further supported by earlier work from Shuster and associates (1982). They examined 2295 patients from two regions: the Carolinas, which had soft water and excessive stone incidence, and the Rockies, which had onerous water and low stone incidence. Home tap water samples from urinary stone patient hospitalizations have been compared with controls. After adjusting for environmental factors, no vital difference between the 2 teams was obtained in tap water calcium, magnesium, and sodium concentrations. An incidental but potentially necessary finding was that those consuming water from a private properly had an estimated relative risk for stone formation of 1. They finally concluded that water hardness ought to be a minor concern with respect to stone formation. FluidRecommendations Volume One mainstay of conservative management is the forced increase in fluid intake to achieve a day by day urine output of at least 2 liters (Borghi et al, 1999). First, the mechanical diuresis that ensues could stop urinary stagnation and the formation of symptomatic calculi. It is more doubtless that the creation of dilute urine alters the supersaturation of stone components. Indeed, Pak and colleagues (1980b) measured in vitro and in vivo results of urinary dilution and found that both significantly reduced the urinary activity product ratio (state of saturation) of calcium phosphate, calcium oxalate, and monosodium urate. Moreover, the formation product ratio-that is, the minimal supersaturation wanted to elicit spontaneous nucleation-of calcium oxalate significantly increased. Researchers on the University of Chicago demonstrated that failure to enhance urine output was one of three very strong predictors of relapse for sufferers followed in a devoted stone clinic (Strauss et al, 1982a). The previously described stone clinic effect has been primarily attributed to increases in fluid consumption and attendant increases in urinary output (Hosking et al, 1983). However, though the idea of increased fluid intake is kind of simple, it can be quite tough to obtain affected person compliance. Anecdotally, most physicians with an curiosity in kidney stone illness have seen that many sufferers are unable to maintain increased urinary output over the long run. In a well-controlled study involving fixed diets and a crossover design, 18 topics with a history of calcium nephrolithiasis drank solely hard water, delicate water, or faucet water (Bellizzi et al, 1999).
Cyproheptadine 4 mg cheap with visa
Isolation from human calcium oxalate renal stones of nephrocalcin allergy symptoms with cough cyproheptadine 4 mg generic free shipping, a glycoprotein inhibitor of calcium oxalate crystal growth: proof that nephrocalcin from sufferers with calcium oxalate nephrolithiasis is poor in gamma-carboxyglutamic acid allergy symptoms clogged ears buy 4 mg cyproheptadine. Clinical and biochemical profile of patients with "pure" uric acid nephrolithiasis compared with "pure" calcium oxalate stone formers. Biochemical variables in pre- and postmenopausal women: reconciling the calcium and estrogen hypotheses. The influence of hyperinsulinaemia on calcium-phosphate metabolism in renal failure. Urinary glycosaminoglycans as risk components for uric acid nephrolithiasis: case management study in a Sardinian genetic isolate. A simple method for the determination of urinary state of saturation with respect to brushite. Comparison of semi-empirical with computer-derived strategies for estimating urinary saturation of calcium oxalate. Comparison of semi-empirical and computer derived strategies for estimating urinary saturation of brushite. Metabolic risk elements in sufferers with ureteropelvic junction obstruction and renal calculi. Mechanism of renal calcium conservation with estrogen substitute therapy in girls in early postmenopause-a scientific analysis middle study. Converting enzyme inhibition causes hypocitraturia independent of acidosis or hypokalemia. Association of absence of intestinal oxalate degrading micro organism with urinary calcium oxalate stone formation. Oxalate toxicity in renal epithelial cells: traits of apoptosis and necrosis. Tamm-Horsfall protein is a crucial renal protection factor protecting in opposition to calcium oxalate crystal formation. The immunological integrity of matrix substance A and its potential detection and quantitation in urine. Transmembrane oxalate exchange: its relationship to idiopathic calcium oxalate nephrolithiasis. Parathyroid hormone receptors and intracellular mediators in command of proximal tubular operate. Claudin-2-deficient mice are faulty within the leaky and cation-selective paracellular permeability properties of renal proximal tubules. Metabolic abnormalities associated with renal calculi in sufferers with horseshoe kidneys. Effect of low-carbohydrate high-protein diets on acid-base stability, stone-forming propensity, and calcium metabolism. Identification and characterization of a gene with base substitutions associated with the absorptive hypercalciuria phenotype and low spinal bone density. Characterization of provider females and affected males with X-linked recessive nephrolithiasis. Importance of delicate hyperoxaluria in the pathogenesis of urolithiasis-new proof from studies in the Arabian peninsula. The distribution of urinary calcium excretions in normal persons and stone-formers. Saturation-inhibition index as a measure of the chance of calcium oxalate stone formation in the urinary tract. Therapeutic motion of citrate in urolithiasis explained by chemical speciation: increase in pH is the determinant issue. Kidney stones: a global picture of prevalence, incidence, and related threat elements. Effects of magnesium deficiency on intratubular calcium oxalate formation and crystalluria in hyperoxaluric rats. The scientific basis of calcium oxalate urolithiasis: predilection and precipitation, promotion and proscription. The definition of the mechanism of hypercalciuria is necessary for the remedy of recurrent stone formers. Successful treatment of hyperuricosuric calcium oxalate nephrolithiasis with potassium citrate. A prospective examine of danger components for nephrolithiasis after Roux-en-Y gastric bypass surgical procedure. Urolithiasis in a rural Wisconsin population from 1992 to 2008: narrowing of the male-to-female ratio. Effect of dietary adjustments on urinary oxalate excretion and calcium oxalate supersaturation in sufferers with hyperoxaluric stone formation. Hypomagnesuric hypocitraturia: an apparent new entity for calcium nephrolithiasis. Renal clearance of [14C]oxalate: comparability of constant-infusion with single-injection techniques. The effect of temperature, humidity and dehydration on the formation of renal calculi. An evaluation of the physicochemical risk for renal stone illness throughout pregnancy. Relation between geographic variability in kidney stones prevalence and danger elements for stones. Factors that predict relapse of calcium nephrolithiasis during treatment: a potential examine. Distribution of osteopontin and calprotectin as matrix protein in calcium-containing stone. Cells of proximal and distal tubular origin respond in another way to challenges of oxalate and calcium oxalate crystals. Effect of vitamin E and mannitol on renal calcium oxalate retention in experimental nephrolithiasis. Idiopathic hypercalciuria and hereditary hypophosphatemic rickets: two phenotypical expressions of a standard genetic defect. Deficiency of the calcium-sensing receptor within the kidney causes parathyroid hormone�independent hypocalciuria. The impact of osteopontin immobilized collagen granules in the seed crystal method. Oxalate measurement in the picomol range by ion chromatography: values in fasting plasma and urine of controls and patients with idiopathic calcium urolithiasis. Suggestive proof for a susceptibility gene near the vitamin D receptor locus in idiopathic calcium stone formation.
Cyproheptadine 4 mg for sale
Current immunosuppression protocols have decreased the speed of biopsyproved acute mobile rejection to 10% to 15% within the first yr allergy medicine 6 hours relief cyproheptadine 4 mg generic fast delivery. The most typical manifesting sign is an increasing serum creatinine and reducing urine output allergy keflex symptoms purchase cyproheptadine 4 mg without a prescription. Symptoms may embody pain, swelling over the graft, malaise, and fever; however these are rare. Imaging studies might reveal decreased cortical blood circulate and tubular function. However, none of those findings is restricted, so needle biopsy of the kidney graft is the current commonplace diagnostic test. The criteria for histologic classification of renal rejection have been standardized at a sequence of conferences in Banff (Solez, 2010). The typical findings in acute mobile rejection are mononuclear infiltration of tubules and vessels. The deposition of complement fragments (C4d) in peritubular capillaries is now recognized as diagnostic of rejection frequently associated with donor-specific antibodies. The histologic options of interstitial fibrosis, arteriolar sclerosis, and tubular atrophy rarely enhance with augmented immunosuppression, and are in some cases the outcomes of drug toxicity. The induction of donor-specific immune tolerance is the holy grail of transplantation. Tolerance would allow the immune system to accept donor organs, without compromising the traditional response to infectious and malignant antigens. The proven fact that tolerance has been achieved in many animal studies but rarely in people underscores the issue in moving this goal from the animal model to precise patients (Sykes, 2009). In profitable hematopoietic cell transplantation, a steadiness between the host versus graft and graft versus host response allows cells from the donor and recipient to coexist. Advances in immunosuppressive medication have improved early graft survival rates, but these enhancements have had little impression on late graft loss, largely due to persistent rejection. The induction of donor-specific immune tolerance would avoid these complications whereas also preventing persistent rejection. Antibodies produced by B lymphocytes can recognize international antigens immediately and are a principal component of the humoral immune response. The molecular mechanisms which may be concerned in the activation and proliferation of lymphocytes are the principal targets for blockade by pharmacologic immunosuppression. ImmunosuppressionProtocols Immunosuppressive protocols in kidney transplantation continue to evolve as our understanding of the biology of the immune response expands and pharmacologic agents to block the response are found. Antibiotics, including antifungal and antiviral medicine, also have permitted extra intensive immunosuppression. Nearly all immunosuppression protocols have been tested in animal models of solid-organ transplantation and then used in people. Some of the protocols have been developed via fastidiously designed clinical trials, but many have been launched in off-label utility by pioneering physicians and patients. In the Nineteen Fifties the first protocols included total-body irradiation and corticosteroids. Shortly after the first profitable equivalent twin transplant, azathioprine permitted graft survival with some dwelling associated donors. Most experimental models achieved superior outcomes if the T-lymphocyte inhabitants might be lowered and allowed to slowly get well. The administration of heterologous polyclonal serum from animals exposed to human immune tissue (antithymocyte globulin) and (antilymphocyte globulin) led to the idea of induction immunosuppression. It was also acknowledged that top doses of corticosteroids and lymphocyte depletion may reverse acute cellular rejection. Unfortunately, the 1-year graft survival was approximately 50%, with as a lot as 20% mortality from infectious issues on this era. In the early Eighties, cyclosporine, a calcineurin inhibitor, was launched and maintenance immunosuppression in combination with azathioprine and prednisolone (triple therapy) improved 1-year graft survival rates to larger than 80%, together with deceased and living-donor kidneys. The success of solid-organ transplantation and the unwanted effects of these medication stimulated the pharmaceutical industry to develop more selective agents to goal the transplant-specific immune response. Immunosuppression protocols are based mostly on the chance for rejection (including donor and recipient factors), minimization of long-term unwanted effects, and cost. The mechanism of motion and toxicity of immunosuppressants are listed in Tables 47-3 and 47-4. Using these brokers, biopsy-proved graft rejection charges are roughly 10% within the first yr and mortality charges proceed to enhance, but approximately 40% of adult recipients turn out to be diabetic. Many of these drugs require continued monitoring of blood ranges as a end result of metabolism could be affected by drug interactions (Box 47-3). The natural course of cytomegalovirus an infection and disease in renal transplant recipients. Despite the absence of cellular rejection, many sufferers will develop antibodies to antigens on the allograft, which is acknowledged as a big risk factor for chronic transplant rejection. Many young sufferers would require a couple of transplant procedure when their first transplant in the end fails. Infection the timing of an an infection after transplantation is critical to the suitable diagnosis and management. Within the primary month the organisms tend to be these causing infections at an establishment in different sufferers with main urologic operations. The most common infections are related to technical complications of surgical procedure and invasive medical gadgets and mostly contain the genitourinary tract. The medical circumstances of the patient, such as diabetes, malnutrition, obesity, irregular urinary tract, and previous infections, improve the chance. Careful preparation of the donor graft, minimal blood loss, brief ischemia time, mobilization of the patient, and immediate elimination of catheters and drains reduces the risks for an infection. All infections ought to be treated with empirical antibiotics and adjusted based on the sensitivity of cultured organisms. During months 1 to 6 after surgery, infections which are managed by the mobile immune system are more prevalent. The incidence of those infections is influenced by the recipient and donor history of preoperative exposure and augmented immunosuppression (Table 47-5). Prophylactic treatment has significantly decreased the morbidity of immunosuppression (Table 47-6). The infections that occur greater than 6 months after transplant are influenced by graft perform, threat for rejection, and former infections. Therapy ought to be based mostly on a complete urologic physical examination and urine culture and sensitivity outcomes. Some patients with minimal pretransplant urine output must be inspired to improve fluid consumption and void incessantly. A voiding diary and assessment of postvoid residual facilitates affected person schooling. If infections are infrequent, antibiotics must be supplied to be initiated by the affected person when signs happen.
Cyproheptadine 4 mg free shipping
Total reconstruction of the penis employing the "cricket bat flap" single stage forearm free graft allergy testing irvine discount cyproheptadine 4 mg fast delivery. Long-term consequence of ventral buccal mucosa onlay graft urethroplasty for urethral stricture repair allergy shots las vegas cyproheptadine 4 mg generic free shipping. Perineal restore of pelvic fracture urethral distraction defects: expertise in one hundred twenty sufferers during the last 10 years. Vessel-sparing excision and primary anastomosis (for proximal bulbar urethral strictures). Perineal anastomotic urethroplasty for managing post-traumatic urethral strictures in youngsters: the long-term consequence. The value of immediate or early catheterization of the traumatized posterior urethra. The technique of vessel sparing excision and first anastomosis for proximal bulbous urethral reconstruction. Dual placement of artificial urinary sphincter gadget and an endoprosthetic for incontinence and bladder neck contracture. Ventral onlay buccal mucosal grafts for anterior urethral stricture: long-term followup. Evaluation and administration of traumatic posterior urethral disruption with versatile cystourethroscopy. Phalloplasty using radial forearm osteocutaneous free flaps in female-to-male transsexuals. Recurrent lichen sclerosus et atrophicus in urethroplasties from a quantity of pores and skin grafts. Long-term end result of forearm flee-flap phalloplasty in the therapy of transsexualism. Comparison of open and endoscopic treatment of posttraumatic posterior urethral strictures. In: Second International Consultation on Sexual Dysfunctions, Co-sponsored by International Consultation on Urological Diseases, International Society of Urology, and International Society for Sexual and Impotence Research. Can end result of internal urethrotomy for brief phase bulbar urethral stricture be predicted Synchronous administration of bladder neck contracture and stress urinary incontinence following radical prostatectomy. Effect of mitomycin C on anterior urethral stricture recurrence after inside urethrotomy. Reconstruction of intensive urethral strictures: round fasciocutaneous penile flap. Indications for transsphincter urethroplasty in patients with main bulbous strictures. Primary anastomosis of the traumatically amputated penis: case report and abstract of literature. Penile reconstruction with a free sensate osteocutaneous fibular flap in the surgical management of the intersex affected person. Lichen sclerosus et atrophicus causing phimosis in boys: a potential research with 5-year follow-up after complete circumcision. Urethral plate salvage with dorsal graft promotes profitable penile flap onlay reconstruction of severe pendulous strictures. Reconstruction of traumatic posterior urethral strictures: consequence evaluation in 82 patients. Proximal bulbar urethroplasty through extended anastomotic approach-what are the limits Fossa navicularis reconstruction: influence of stricture size on outcomes and assessment of prolonged meatotomy (first stage Johanson) maneuver. Cadaveric anatomy of pelvic fracture urethral distraction injury: most injuries are distal to the external urinary sphincter. The function of delayed main restore within the acute administration of pelvic fracture accidents of the urethra. The musculo-cutaneous flap technique: an instantaneous and heroic substitute for the strategy of delay. Internal urethrotomy within the management of anterior urethral strictures: long-term followup. Reconstruction of the perineal urethra with a free full thickness skin graft from the prepuce. Construction of male genitalia within the transsexual, utilizing a tubed groin flap for the penis and a hydraulic inflation device. Appendix B: requirements of care: the hormonal and surgical sex reassignment of gender dysphoric individuals. The use of bladder mucosa and combined bladder mucosa/preputial pores and skin grafts for urethral reconstruction. Early endoscopic realignment as main therapy for complete posterior urethral disruptions. Spirochetal forms within the dermal lesions of morphea and lichen sclerosus et atrophicus. Primary urethral reconstruction: the cost minimized strategy to the bulbous urethral stricture. Use of the Wallstent endourethral prosthesis within the treatment of recurrent urethral strictures. Traitement des stenoses uretrales compliquees par suture uretrale bout-a-bout et ureteroplastie par greffe libre du prepuce. North American Study Group: 11-year end result evaluation of endourethral prosthesis for the remedy of recurrent bulbar urethral stricture. Lingual versus buccal mucosa graft urethroplasty for anterior urethral stricture: a potential comparative evaluation. Anastomotic urethroplasty for failed beforehand handled membranous urethral rupture. The incidence and causes of erectile dysfunction after pelvic fractures associated with posterior urethral disruption. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. Outpatient therapy for male urethral strictures-dilatation versus inside urethrotomy. Balanitis xerotica obliterans (post operationem) und ihre beziehungem zur Kraurosis glandis et preaeputii. Biologic destiny of autogenous vein implants as arterial substitutes: scientific, angiographic and histopathologic observations in femoro-popliteal operations for atherosclerosis. Use of multiple UroLume endourethral prostheses in advanced bulbar urethral strictures. Do some patients with morphea and lichen sclerosus et atrophicus have a Borrelia an infection Radial urethrotomy and intralesional mitomycin C for the administration of recurrent bladder neck contractures. Long-term follow-up for reconstruction of strictures of the fossa navicularis with a single approach.
Cyproheptadine 4 mg generic
Biology of ischemic and poisonous renal tubular cell injury: position of nitric oxide and the inflammatory response new allergy treatment 2013 cyproheptadine 4 mg mastercard. Rapidly progressive glomerulonephritis: present and evolving therapy methods allergy testing athens ga cyproheptadine 4 mg online buy cheap. The low delivery weight hypothesis as a plausible rationalization for the black/white variations in hypertension, non-insulindependent diabetes, and end-stage renal illness. Low-flux versus high-flux synthetic dialysis membrane in acute renal failure: potential randomized research. Mechanisms contributing to musclewasting in acute uremia: activation of amino acid catabolism. Dissociation of tubular cell detachment and tubular cell demise in clinical and experimental "acute tubular necrosis. Minimizing danger of nephrogenic systemic fibrosis in cardiovascular magnetic resonance. The decline in residing kidney donation in the United States: random variation or cause for concern Nephrotoxicity of ionic and nonionic distinction media in 1196 sufferers: a randomized trial. Mortality caused by sepsis in patients with end-stage renal illness compared with the overall population. Impaired pulmonary oxygenation of diabetic origin in patients undergoing coronary artery bypass grafting. Progression of chronic kidney disease in youngsters with vesicoureteral reflux: the North American Pediatric Renal Trials Collaborative Studies Database. Glomerular quantity and size in relation to age, kidney weight, and physique surface in normal man. Fenoldopam and renal operate after partial nephrectomy in a solitary kidney: a randomized, blinded trial. The function of N-acetylcysteine in the prevention of contrast-induced nephropathy in sufferers undergoing peripheral angiography: a structured evaluation and meta-analysis. Role of hypoalbuminemia and hypocholesterolemia as copredictors of mortality in acute renal failure. Frequency, etiology and remedy of childhood end-stage kidney disease in Australia and New Zealand. Nephrology forum: apoptotic regulatory proteins in renal harm [clinical conference]. Prognosis of sufferers with acute renal failure requiring dialysis: results of a multicenter examine. The impact of dietary protein restriction on the progression of diabetic and nondiabetic renal diseases: a metaanalysis. Gadolinium-contrast toxicity in patients with kidney illness: nephrotoxicity and nephrogenic systemic fibrosis. Imaging patients with kidney illness: how can we approach contrast-related toxicity Acute renal failure in critically sick sufferers: a multinational, multicenter research. An evaluation of an integrative care approach for end-stage renal disease patients. Rhabdomyolysis and myogloginuric acute renal failure in the lithotomy/exaggerated lithotomy position of urogenital surgical procedures. Localization of proliferating cell nuclear antigen, vimentin, c-Fos, and clusterin in the postischemic kidney: evidence for a heterogenous genetic response among nephron segments, and a large pool of mitotically energetic and dedifferentiated cells. Dopamine remedy for sufferers vulnerable to renal dysfunction following cardiac surgical procedure: science or fiction Intravascular administration of mannitol for acute kidney damage prevention: a systematic evaluation and meta-analysis. Matrix metalloproteinases contribute to kidney fibrosis in chronic kidney ailments. Atrial natriuretic peptide protects towards acute ischemic renal failure in the rat. Enhanced recovery from acute renal failure by the postischemic infusion of adenine nucleotides and magnesium chloride in rats. Combination therapy with octreotide, midodrine, and albumin improves survival in sufferers with type 1 and type 2 hepatorenal syndrome. Acute renal failure in critically ill sufferers: prognosis for recovery of kidney operate after prolonged dialysis help. Ion-exchange resins for the therapy of hyperkalemia: are they safe and efficient Evaluation of the modification of diet in renal disease study equation in a big diverse inhabitants. Fenoldopam mesylate for the prevention of contrast-induced nephropathy: a randomized controlled trial. The position of the B7 costimulatory pathway in experimental chilly ischemia/reperfusion damage. Prevention of radiographiccontrast-agent-induced reductions in renal operate by acetylcysteine [see comments]. Percutaneous revascularization for ischemic nephropathy: the previous, current, and future. Relative risk and economic consequences of inpatient care among patients with renal failure. Reversible renal insufficiency due to angiotensin changing enzyme inhibitors in hypertensive nephrosclerosis [see comments]. Dialysis therapies had been initially indicated just for patients with acute kidney damage. In the primary half of the century there were only short-term success and plenty of technical failures with kidney transplantation. Through transplantation experiments in animal fashions lots of the fundamentals of immunology have been elucidated. During the Second World War the remedy of burns stimulated intense curiosity in pores and skin grafting. A sequence of papers beginning in 1944 by Peter Medawar clearly demonstrated the method of graft rejection, as properly as the acceptance of tissue from the same particular person or an similar twin. Moreover, elegant experiments demonstrated that rejection might be prevented by switch of cells from the donor to the recipient through the neonatal interval (Billingham et al, 1953). Advances in vascular surgical approach and tolerance induction renewed interest in organ transplantation. Hartwell Harrison (urology) on the Peter Bent Brigham Hospital performed the first successful kidney transplant between equivalent twins in December 1954 (Terasaki, 1991; Starzl, 1992). Transplantation has evolved from an experimental process to the standard of care for a lot of forms of organ failure. Urologists will subsequently continue to be referred to as on to manage patients with organ transplants. Blood is removed using a catheter in a central vein or large-bore needles inserted into an arteriovenous fistula/graft. Fluid elimination, also identified as ultrafiltration, is controlled by regulating the hydrostatic strain throughout the membrane. Increasing the variety of therapies per week and decreasing the speed of fluid elimination could decrease signs, but is usually restricted to these patients with a devoted caregiver who can administer the therapy within the house. Permanent dialysis access using an arteriovenous fistula has one of the best patency fee and reduces the risk for hematogenous an infection. Venous stenosis and eventual lack of vascular entry is an increasingly recognized complication of extended dialysis utilizing central venous catheters.
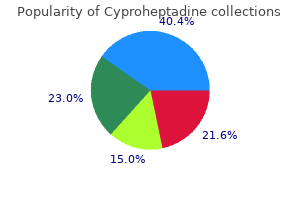
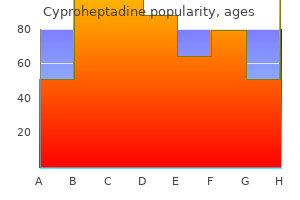
Real Experiences: Customer Reviews on Cyproheptadine
Osmund, 39 years: It is unclear whether or not the tumor biology or distinction in care of aged sufferers is answerable for this remark.
Roy, 50 years: Norepinephrine vasoconstricts all the main vascular beds within the kidney, mediated by way of the 1 receptor.
8 of 10 - Review by S. Trano
Votes: 60 votes
Total customer reviews: 60
