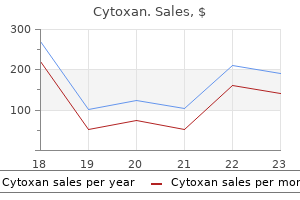
Cytoxan dosages: 50 mg
Cytoxan packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy cytoxan 50 mg cheap
In order to obtain an sufficient distal margin (2 cm) with sphincter preservation symptoms women heart attack cytoxan 50 mg visa, the decrease border of a tumor should be situated excessive enough above the highest of the anorectal ring medicine to calm nerves cytoxan 50 mg cheap line. Although a patient may assume that a colostomy signifies a hopelessly incurable cancer, we must emphasize that the colostomy is important because of the anatomic location, not essentially the severity of the rectal cancer. Vascular Supply Arteriography demonstrates intensive intramural anastomoses between the superior, center, and inferior rectal arteries. Because the venous methods communicate, low rectal cancers may spread by way of the portal and systemic circulations. Lymphatic Drainage Local recurrence after resection is frequent and can happen with and with out distant metastatic illness. Chapter 40 Cancer of the Rectum Superior hypogastric plexus 837 can unfold regionally via lymphatics that observe cranially alongside the superior hemorrhoidal vessels. Heald has described a "zone of downward unfold" within the mesorectum3; this zone can encompass as a lot as 4 cm beyond the distal mucosal fringe of the tumor. Appreciation of the zones of upward and downward unfold has in uenced the extent of dissection surgeons now perform for healing resection of rectal cancers. Lymph from the lower rectum may drain into the inferior mesenteric system or into the network along the center and inferior rectal arteries, posteriorly along the middle sacral artery, and anteriorly through the channels to the retrovesical or rectovaginal septum, to the iliac nodes, and in the end, to the periaortic nodes. In a Japanese research, the obturator nodes, external to the hypogastric nerve plexus, were discovered to be concerned with cancer in 8% of tumors situated in the distal rectum, whereas these nodes were hardly ever, if ever, involved with proximal tumors. A from the anal canal above the dentate line usually drain via the superior rectal lymphatics to the inferior mesenteric lymph nodes and laterally to the obturator and internal iliac nodes. Below the dentate line, lymph drains primarily to the inguinal nodes however may empty into the inferior or superior rectal lymph nodes. Sympathetic nerves originate from L1�L3, form the inferior mesenteric plexus, travel through the superior hypogastric plexus, and descend as the hypogastric nerves to the pelvic plexus. Fibers from this plexus innervate the rectum in addition to the bladder, ureter, prostate, seminal vesicles, membranous urethra, and corpora cavernosa. Fascial Planes e walls and oor of the pelvis are covered by the endopelvic, or parietal, fascia. With this info, surgeons should individualize the treatment and care of each patient. History e affected person with rectal cancer normally presents to the surgeon after a de nitive endoscopic prognosis. Speci c signs might assist the surgeon in deciding on the optimum strategy to therapy. Information pertaining to anal sphincter perform is invaluable when one is contemplating a low anastomosis. Preoperative sexual operate is necessary to know because one must talk about the dangers of the procedure and potential diminution of sexual operate postoperatively. A complete medical history should be geared toward identifying different medical conditions, corresponding to cardiopulmonary, renal, and nutrition, that will require additional analysis earlier than surgical intervention and allow appropriate risk stratication. For patients with a cardiac historical past or signs, a stress take a look at and cardiology evaluation are indicated. Women should bear a complete pelvic examination so as to decide vaginal invasion or spread to the ovaries. Accurate preoperative staging is gaining rising importance as combined-modality remedy and sphincter-preserving surgical approaches are considered. Ureteral involvement by the tumor could be assessed and permits for planning of ureteral stent placement preoperatively. Rigid proctoscopy can also be important to the analysis of sufferers with rectal most cancers because it demonstrates the proximal and distal ranges of the mass from anal verge; extent of circumferential involvement; orientation within the lumen; and relationship to the vagina, prostate, or peritoneal re ection. Furthermore, a mass will usually be described as being a sigmoid or rectosigmoid tumor on exible colonoscopy, and, when the affected person is evaluated within the o ce with inflexible sigmoidoscopy, the lesion is usually found to be much lower and actually is usually a real rectal most cancers that quali es for neoadjuvant chemoradiotherapy. A full colonoscopy to the cecum is essential to rule out synchronous cancers, which occur 2�8% of the time. Localized cancers involving only the mucosa and submucosa often may be distinguished from tumors that penetrate the muscularis propria or prolong by way of the rectal wall into the perirectal fat. Staging by scientific examination, radiology, and pathology aids in planning remedy, evaluating response to remedy, comparing the results of varied treatment regimens, and figuring out prognosis. Depth of invasion (T stage) of the first tumor is a crucial prognostic variable as rising depth of invasion is correlated with an growing chance of lymph node metastases. For occasion, early-stage cancers extending into the muscularis mucosa (T1) will have a 10�13% incidence of metastasizing to perirectal lymph nodes. Large arrow demonstrates ngerlike projections of carcinoma invading into the mesorectal fats. Super cially invasive, small cancers may be managed e ectively with local excision. Yet others current with regionally superior tumors adherent to adjoining constructions such as the sacrum, pelvic sidewall, vagina, uterus, cervix, prostate, or bladder, requiring an much more in depth operation. After establishing the analysis and completing the staging workup, a choice is made whether or not to pursue quick resection or administer preoperative chemoradiotherapy. Bowel Preparation e high bacterial load in the intestinal tract requires preoperative bowel decontamination to scale back the incidence of infectious problems. Prior to the routine use of mechanical bowel preparation and preoperative antibiotics, the reported price of infection following colorectal surgery was 60%. In two separate surveys of North American colorectal surgeons, almost two-thirds most well-liked the polyethylene glycol electrolyte options due to the reliability of the cleaning outcomes. Studies have shown that mechanical bowel preparation supplies little, if any, extra bene t to lowering the perioperative infection fee. However, we still recommend to our sufferers that a mechanical bowel preparation be carried out in massive part because it permits for simpler manipulation of the colon and rectum with both open and laparoscopic surgery. Poorly di erentiated cancers have a worse long-term prognosis than well- or moderately di erentiated tumors. Other factors that portend a poor prognosis embody direct tumor extension into adjacent buildings (T4 lesions); lymph node metastases; lymphatic, vascular, or perineural invasion; and bowel obstruction. Following a potentially healing resection, the 5-year survival price varies in accordance with illness extent22,23 (Table 40-4). However, these survival gures might enhance with the increased use of adjuvant remedy. Instead of an oral antibiotic preparation most surgeons use perioperative systemic antibiotics. A typical option to cover both aerobic and anaerobic intestinal bacteria is cefazolin and metronidazole administered intravenously just prior to the skin incision. Postoperative antibiotic prophylaxis usually is sustained for 24 hours, although the perioperative dose is extra crucial. Some surgeons do "double" prophylaxis with oral and systemic antibiotics in all surgeries beneath the peritoneal re ection. Perioperative systemic antibiotic protection is broadened in sufferers with high-risk cardiac lesions similar to prosthetic coronary heart valves, a previous history of endocarditis, or a surgically constructed systemic-pulmonary shunt and with intermediate-risk cardiac lesions corresponding to mitral valve prolapse, valvular heart disease, or idiopathic hypertrophic subaortic stenosis. Vancomycin is substituted for ampicillin if the patient is allergic to penicillin or cephalosporin.
Best cytoxan 50 mg
Broths are often incubated for a minimal of 5 days and examined daily for turbidity treatment 1st line 50 mg cytoxan cheap with amex. May include selective dietary supplements MacConkey agar is a selective medium for the isolation of coliforms similar to Escherichia coli medicine queen mary generic cytoxan 50 mg with visa. This medium incorporates bile salts that are inhibitory for so much of organisms, and permits lactose and non-lactose fermenting micro organism to be distinguished Enriched fluid media. Bacteriology Laboratory Tests ninety seven Bacteria Enterococci Beta-haemolytic streptococci Alpha-haemolytic streptococci Streptococcus pneumoniae Staphylococci (all types) Haemophilus influenzae Neisseria meningitidis Neisseria gonorrhoeae Coliforms (Escherichia coli, Klebsiella spp. MacConkey (enteric organisms) and Sabouraud (fungi) are examples of selective media. From a liver abscess, up to three various varieties of bacteria would warrant every isolate being recognized and antibiotic susceptibility testing. It is essential at this stage that the microbiologist discusses these findings with the scientific group, so as to determine what further work would aid management of the affected person. There ought to be methods in place to allow all specimens to have their initial processing on the day of receipt (day 0). All blood culture units should be placed within the blood tradition machine inside 4 hours of being taken from the affected person. When the medical team are contemplating such organisms within the differential prognosis, they should be in dialogue with the microbiologist at the earliest opportunity to ensure that the correct laboratory process is followed. The number of bacterial colonies/L of urine can also be recorded, with >108/L being thought-about vital. In order to speciate these organisms, single exams such as those outlined below are used. The Escherichia coli, Salmonella and Shigella plates are incubated at 37�C for twenty-four hours, while the Campylobacter plate is incubated for 48 hours in a microaerophilic setting to optimize recovery. In addition, a portion of the stool sample is inoculated into selenite broth, a selective enrichment broth for Salmonella. A er 18 hours this is subcultured onto agar medium to get well Salmonella that has grown. Antibiotics could also be used in therapy, with the exception of shiga toxin-producing Escherichia coli. Differentiation of streptococci and staphylococci the catalase test is used to differentiate streptococci (catalase-negative) from staphylococci (catalase-positive). Bacteriology Laboratory Tests a hundred and one bacteria convert the peroxide to water and gaseous oxygen. Coagulase is an enzyme that is ready to clot plasma in a style similar to the thrombin-catalyzed conversion of fibrinogen to fibrin. The take a look at is essential in differentiating Staphylococcus aureus from the coagulase-negative staphylococci such as Staphylococcus epidermidis, the widespread skin commensals. The presence of a coagulase-negative staphylococcus in blood tradition would often be thought-about a pores and skin contaminant, whereas Staphylococcus aureus prompts a reassessment of the affected person to decide the attainable supply and confirm the proper antibiotic treatment. The Oxoid Staphytect check uses blue coloured latex beads coated with protein A, fibrinogen and antibodies to the cell wall polysaccharide of Staphylococcus aureus. However, Staphylococcus aureus cross-links the beads by Bubbles of oxygen Identification of streptococci - and -haemolysis step one in the classification of streptococci is their haemolytic nature as exhibited on blood agar. Many micro organism produce haemolysins, that are extracellular proteins secreted by the cells that degrade lipid membranes. The membrane of pink blood cells is also degraded and the lysis of those cells may be seen on blood agar plates. Streptococcus pneumoniae is delicate to the chemical optochin, whereas the rest of the -haemolytic streptococci are resistant to this compound. Capillary tube filled with hydrogen peroxide Dab base onto colony growing on agar plate Positive No bubbles Negative Lancefield grouping of the -haemolytic streptococci the -haemolytic streptococci are further subdivided on the premise of their cell wall polysaccharide. The soluble extract is mixed with latex beads coated with group-specific antibodies; an agglutination reaction identifies the group the isolate belongs to . There are six major teams of -haemolytic streptococci, termed A, B, C, D, F and G, and inside these there are a selection of essential pathogens, including group A streptococcus, Streptococcus pyogenes, group B streptococcus, Streptococcus agalactiae and group C streptococcus, Streptococcus dysgalactiae. The -haemolytic organism is sensitive to optochin (Op) and to oxacillin (Ox), figuring out the isolate as a penicillin-sensitive pneumococcus. X and V test Colony combined with cell wall extraction reagent (enzyme or acid) and incubated at 37 C for half-hour this easy take a look at is used to differentiate Haemophilus influenzae from different haemophilus species. Chocolate agar is blood agar the place the medium has been heated to 80�C Extracted polysaccharide in suspension Blotting paper soaked in oxidase reagent (aqueous solution of tetramethyl phenylenediamine dihydrochloride) Extract blended with suspensions of latex beads each coated with a specific antipolysaccharide antibody. A optimistic antibody�antigen reaction is proven by clumps and identifies the group; in this instance, group A streptococcus or Streptococcus pyogenes. As with gram-positive bacteria, gramnegative organisms can be categorized utilizing easy exams. Colony smeared onto soaked blotting paper Colour develops inside 30 seconds Negative Positive Oxidase test Gram-negative bacteria could be divided into oxidase-positive and oxidase-negative. Cytochrome c is ready to convert the colourless oxidase reagent to a blue color, figuring out the organism as oxidase positive. The take a look at depends on putting paper discs containing both X or V issue and a disc containing both elements on a primary medium such as nutrient agar. While trendy transport swabs do maintain a variety of labile organisms viable, pus is the better pattern. If further testing is required, for instance for mycobacteria, pus is a superior specimen to process for this objective. Haemophilus influenzae is recognized by growth across the disc that incorporates both X and V. As bacteria are capable of metabolize (ferment) sure sugars to acids, progress (turbidity) or a color change within the medium from alkaline to acid can be utilized to determine which sugars a specific organism makes use of. The expression of an enzyme such as urease and the detection of end-products of metabolism corresponding to indole, a product of tryptophan metabolism, are different tests used. The organism here is Escherichia coli, which ferments all however two of the sugars, and amongst other test results is indole-positive. Here the first carbohydrate well (glucose) can be used for the nitrate reduction check. A cassette containing a variety of cells, each with one concentration of an antibiotic, is inoculated with a dilute suspension of the organism. In the machine, Relative amount the organism from a tradition plate is combined with a matrix substance corresponding to sinapinnic acid, a phenyl propanol. This process takes place in a vacuum, and the ionized elements are accelerated by way of an electric subject generator and journey through the vacuum at a rate proportional to their mass. The detector gives a qualitative and quantitative readout of the proteins that have been in the sample. The complicated aggregation of proteins that make up the ribosomes of the cell are dominant.
Syndromes
- Vision loss
- CBC possibly showing low hematocrit
- Meat or poultry may come into contact with normal bacteria from the intestines of an animal while it is being processed
- Tiredness
- Rapid heart rate
- Myocarditis
Generic cytoxan 50 mg otc
In contrast medications covered by medicaid cytoxan 50 mg cheap free shipping, the persistence of extreme reflux signs while on medicine signifies incomplete acid suppression medications like tramadol 50 mg cytoxan cheap mastercard. The persistent acidic gastric juice causes bile acids to precipitate out of solution. This nullifies their effect, therefore less or no intestinal metaplasia or adenocarcinoma. Indeed, the share of sufferers presenting with an early T1 N0 adenocarcinoma has increased over time and, within the newer years, account for nearly 50% of all resected tumors. In the new staging system cancers of the gastric cardia that reach into the gastroesophageal junction are classified as adenocarcinomas of the esophagus rather than the abdomen. This is an improvement however nonetheless is imprecise as a result of the shortcoming to consistently define the placement of the gastroesophageal junction. In 2000, the Association of Directors of Anatomic and Surgical Pathology defined the gastroesophageal junction as a horizontal line drawn throughout the end of the tubular esophagus at the level the place it begins to flare into the stomach. We have suggested that the location of the gastroesophageal junction is de ned more accurately by histology because the proximal limit of gastric oxyntic mucosa. Such lesions must be eliminated by endoscopic mucosal resection to determine the nature of the lesion and, if a most cancers, its depth of penetration into the esophageal wall. To handle these patients appropriately requires that surgeons turn out to be adept at endoscopy and endoscopic mucosal resection. Further, its late morbidity, together with weight reduction, dumping, and diarrhea, is signi cantly less. If a recurrence happens, a pharyngolaryngoesophagectomy is performed as a salvage procedure. It is important that these patients understand this method prior to treatment and are prepared to submit to yearly surveillance after the de nitive radiochemotherapy. Fit sufferers with tumors within the decrease cervical or upper thoracic esophagus are treated with cytoreduction of the tumor by radiochemotherapy adopted by resection and reconstruction with a free jejuno-interposition. Fit patients with tumors in the mid or decrease thoracic esophagus, gastroesophageal junction, or gastric cardia are handled with an en bloc esophagectomy and full lymphadenectomy. After elimination, the recent specimen contracts to approximately 50% of its length or down to 5 cm of grossly normal appearing esophagus. Similarly, you will need to have a larger than l-mm free circumferential radial margin on the specimen after a curative resection. When analyzed by Cox regression, the variety of lymph nodes eliminated modeled as a steady variable was the third most important prognostic factor behind the variety of involved nodes and the depth of tumor invasion. Of the three factors, the number of nodes eliminated is the one predictor of survival that may be in uenced by the surgeon. I am not convinced that adding a 3rd eld, that may be a cervical node dissection, improves the survival su ciently to overcome the elevated morbidity. An exception to this policy is when unsuspected concerned recurrent laryngeal nodes are discovered while performing the neck dissection in the course of the preliminary operation in preparation for a neck anastomosis. In this case a cervical node dissection is added to the initial operation to take away recurrent laryngeal and deep cervical nodes on the left. In a unique study, the en bloc and transhiatal resections had been in contrast utilizing a retrospective case-control examine of nonrandomized patients with similar-size transmural tumors (T3) and lymph node metastasis chosen at random from our registry. When this data was applied to the 5-year outcome of the only randomized research accomplished to examine the 2 resections, solely those sufferers with one to eight involved lymph nodes signi cantly bene ted from an en bloc resection. Based on these research, the en bloc resection is more than likely to bene t sufferers with eight or fewer lymph nodes concerned. Beyond this number the likelihood of systemic disease approaches 100 percent, and neither an en bloc nor a transhiatal resection supplies a long-term bene t. Factors recognized to contribute to this complication are diabetes, hypertension, cardiac arrhythmia, chronic obstructive pulmonary illness, and neoadjuvant therapy. Indeed, I consider that conduit ischemia is the "Achilles heel" of a profitable esophageal resection and reconstruction. When faced with a worrisome ischemic conduit, we pull the conduit up and anchor it within the neck with out performing the anastomosis. A Prolene stitch is placed into the conduit and introduced out to the subcutaneous tissue for a information to nd the conduit on the time of delayed reconstruction. Ninety days after the esophagectomy, a cervical esophagogastrostomy is performed via the unique neck incision. At the time of reconstruction, all had well-perfused gastric conduits and the delayed anastomosis healed and not utilizing a leak, wound infection, or sepsis. True, distant failure stays a significant downside in sufferers with advanced cancer, and a seek for more e ective systemic medicine as properly as a technique to select the right medication for the proper affected person must be supported and inspired. I agree with Dr Law that at present the results of neoadjuvant chemoradiation remedy are con icting, and that printed meta-analysis present minimal to no bene t. Despite this, neoadjuvant chemoradiation is extensively practiced within the United States. A limitation of the current randomized trials is the dearth of correct staging prior to randomization. If randomization is finished accurately, major identified factors that a ect survival, similar to stage of disease, have to be evenly distributed within the research teams prior to randomization because the concept of randomization is used solely to handle unknown components that a ect survival. I have concluded that the research accomplished to date have proven neoadjuvant remedy to be solely e ective in causing cytoreduction of the primary tumor. I would suggest that future neoadjuvant research be accomplished only on sufferers of comparable stage based on fastidiously accomplished pretreatment minimally invasive surgical staging. My concern is that our failure to centralize esophageal surgery in the United States, as is at present being done in England, will relegate surgical therapy from a major position in esophageal most cancers to an adjuvant position. Dr Wee and Dr Sugarbaker present a wonderful description of the en bloc esophagogastrectomy carried out via what is named the tri-incision or McKeown method. We begin in the proper chest by dividing the intercostal veins as they be part of the azygos vein from the arch down to the diaphragmatic hiatus. We then dissect out the intercostal arteries and follow them to the place they be a part of the aorta. We additionally skeletonize the superior and anterior wall of the common and proper hepatic artery, the superior and inferior wall of the portal vein, and the superior and anterior wall of the splenic artery out to the splenic hilum. Skeletonizing the inferior wall of the portal vein is done by using a vein retractor to displace the vein caudally and using the cautery alongside the superior border of the pancreatic head. To their credit they seem to not have restricted the extent of the resection to accommodate the new strategy however somewhat creatively altered their method to keep the extent of the dissection. When that time is reached, some nice benefits of a minimally invasive procedure will diminish and the world of surgical procedure will proceed to do such a process openly until additional technological developments happen that can allow us to go additional in our quest for "user-friendly" surgery. Gastroesophageal re ux illness symptom severity, proton pump inhibitor use, and esophageal carcinogenesis. Vagal-sparing esophagectomy: the best operation for intramucosal adenocarcinoma and Barrett with high-grade dysplasia. Superiority of prolonged en bloc esophagogastrectomy for carcinoma of the decrease esophagus and cardia.
50 mg cytoxan with visa
Clinical considerations and therapeutic strategy for sigmoid volvulus in the aged: a study of 33 circumstances symptoms viral infection cytoxan 50 mg order on-line. Feasibility of single-stage resection and primary anastomosis in sufferers with acute noncomplicated sigmoid volvulus medications you can buy in mexico discount cytoxan 50 mg on line. A comparability of emergency resection and staged administration in perforated diverticular illness. Emergency surgery for diverticular illness sophisticated by generalised and faecal peritonitis. One-stage process in non-elective surgery for diverticular disease problems. Prospective examine of primary anastomosis following sigmoid resection for suspected acute complicated diverticular disease. Meta-analysis of randomised clinical trials of colorectal surgical procedure with or without mechanical bowel preparation. Systematic review of the quick time period outcome of laparoscopic resection for colon and rectosigmoid cancer. Laparoscopic peritoneal lavage for generalized peritonitis due to perforated diverticulitis. Laparoscopic strategy to remedy of sigmoid diverticulitis: adjustments within the spectrum of indications and results of a potential, multicenter research on 1,545 patients. Current medical and surgical treatment is e ective at controlling the illness, however even with optimal remedy recurrences and relapses are frequent. To add to the general complexity, there are numerous therapeutic options that should be tailored to every individual affected person and to every web site of involvement to obtain optimum outcomes. In 1761, Morgagni described a case of an in amed ileum with perforation and thickened mesentery in a young man with a historical past of diarrhea and fever. Initially, many thought that the disease was considered one of each the bowel and the mesentery and, much like malignancies, extensive excision with radical dissection of the mesentery was believed to be one of the only ways to present for the optimal long-term outcome. It additionally appears to be slightly more frequent in girls than in males, although a slight male predominance has been reported in some populations. To date, no speci c major defect in the systemic or mucosal immune system has been identi ed. Lymphoid aggregates could prolong past the mucosa and could be found throughout the muscularis propria. Further progression results in a serpiginous community of linear ulcerations that encompass islands of edematous mucosa producing the basic "cobblestone" look. Mucosal ulcerations may penetrate through the submucosa to type intramural channels that may bore deeply into the bowel wall and create sinuses, abscesses, or stulas. As the in ammation turns into continual, brotic scarring develops and the bowel wall becomes thickened and leathery in texture. Once brostenotic areas become symptomatic, signi cant improvement rarely occurs and surgical intervention is often required. In ammatory response across the advancing sinus tract usually leads to adhesion to surrounding buildings. Typically, perforating illness is accompanied by a degree of stricture formation, but the stula or abscess generated by the perforating component of the illness dominates the clinical image. In the next few paragraphs the in uence of illness sample and location is described. It is mostly the predominant sample of disease that determines the medical presentation and a ects the therapeutic options. Pain related to partial obstruction is generally postprandial and crampy in nature; pain from septic complications is typically steady and associated with fevers. Weight loss is usually associated to meals avoidance, but in extreme circumstances it could be the outcome of malabsorption. With disease of the small intestine, patients might develop a palpable mass, usually located in the right decrease quadrant, related to an abscess or phlegmon in perforating disease or a thickened loop of gut in obstructive illness. Evidence of stulization to the pores and skin, urinary bladder, or vagina may also be elicited with an correct history and physical examination. Joint problems corresponding to ankylosing spondylitis, sacroiliitis, and seronegative polyarteritis can happen. Stricturing of the colon with extra superior disease may give rise to colonic obstruction. As famous beforehand, generally the onset of illness is gradual with the commonest complaints being intermittent stomach pain, bloating, diarrhea, nausea, vomiting, weight loss, and fever. In some instances the onset of signs may be extra sudden, with sufferers relating a history paying homage to acute appendicitis. In these circumstances, ache in the best decrease quadrant may have been current only for a couple of hours or days. A digital rectal examination ought to assess for the presence of anal strictures, ssures, and rectal mucosal ulcerations. Small bowel distinction studies can also provide information relating to enlargement of the mesentery, in addition to formation of an in ammatory mass or abscess. Such ndings are demonstrated by a general mass e ect separating and displacing contrast- lled loops of small gut. It is important to observe, however, that small bowel radiography may not establish all such lesions. Additionally, small bowel studies might not reveal all of the areas of illness with signi cant strictures. Such a distinction offers priceless information concerning the value of medical remedy versus early surgical intervention, as in ammatory stenoses are likely to reply to medical therapy while brotic strictures are greatest handled with surgical procedure. Images from the capsule endoscopy can detect refined mucosal lesions that may not be obvious on small bowel x-rays. Upper endoscopy is useful within the analysis of mucosal lesions of the esophagus, stomach, and duodenum; it also simply identi es strictures and grades their severity. Selecting the optimum medical treatment for every individual requires experience and special experience due to the variable course of the illness, the myriad of di erent clinical shows and related complications, and the will to optimize medical treatment for every medical situation. Other problems which are throughout the di erential prognosis embody radiation enteritis, Yersinia infections, intestinal harm from nonsteroidal anti-in ammatory agents, intestinal tuberculosis, and small bowel tumors. Among crucial ailments to consider are small bowel malignancy and intestinal tuberculosis. In patients in whom small bowel malignancy is suspected, resection must be undertaken to make sure the prognosis. Because in iximab is a potent immunosuppressive agent, issues have been raised about the risk for poor wound healing and postoperative septic issues. Current available data on the perioperative risks related to in iximab are considerably con icting. With the exception of metronidazole, every considered one of these brokers requires a whole and complicated knowledge of applicable dosing, aspect e ects, and therapeutic e cacy, which is beyond the scope of this chapter. Metronidazole is indicated within the maintenance therapy of persistent perineal septic issues and in the remedy of bacterial overgrowth associated with chronic obstructive illness of the small bowel.
Buy cytoxan 50 mg on-line
Although recurrence could also be seen on the distal margin of the anastomosis treatment 3rd nerve palsy 50 mg cytoxan cheap amex, most develop from residual cancer on the pelvic wall symptoms 0f kidney stones 50 mg cytoxan quality. Removal of the rectum and urinary bladder with surrounding lymphatic tissue results in a everlasting colostomy and ileal conduit. Surgical resection combined with aggressive multimodality remedy is advocated to avert the morbidity of pelvic illness and to extend survival in a subset of sufferers, with survival rates up to 30%. Miner and colleagues demonstrated that in sufferers who underwent surgery with palliative intent, improvement was noted in 40% with bleeding, 70% with obstruction, and 20% with pain. Disadvantages embrace radiating the neorectum and small bowel and a lower tendency of sufferers to complete their radiation. While not certainly one of the trials within the Eighties and Nineteen Nineties demonstrated elevated survival, one study did present a lower in native recurrence. Neoadjuvant Chemoradiation ere are a number of potential advantages for utilizing neoadjuvant chemoradiation. Additional advantages include radiating tissues with a larger oxygen supply, not radiating the anastomosis, and decreased chance of growing radiation enteritis as a end result of small bowel is less prone to enter the pelvis. Finally, patients are more likely to full the course of radiation therapy as a end result of it precedes their surgical resection. Furthermore, a meta-analysis concluded that preoperative radiation remedy plus surgical procedure compared with surgical procedure alone signi cantly decreased the 5-year total mortality price, cancer-related mortality fee, and native recurrence price. Despite the preponderance of distal tumors in the preoperative chemoradiation group, there was no difference in general survival or disease-free survival at four years. On the other hand, sufferers receiving preoperative chemoradiotherapy had a 6% local recurrence rate as compared to a 13% native recurrence rate in these receiving postoperative chemoradiotherapy. A theoretical purpose to use postoperative radiation remedy is that more Chapter 40 Cancer of the Rectum 865 preoperative chemoradiotherapy had the next incidence of sphincter preservation and lower treatment-related toxicities (27 vs 40%). Di erences in local recurrence, sphincter preservation, and treatment toxicities were all statistically signi cant. A Polish rectal cancer trial from 2004 compared preoperative short-course radiotherapy (5 days of 5 Gy) versus conventional radiotherapy (28 fractions of 1. However, sphincter preservation within the short-course group was 61% and within the long-course group 58%. Furthermore, this Polish trial reported no di erences in anorectal or sexual perform between the short- or long-course radiotherapy. In the patients who acquired pre-op, post-op, or pre-op and post-op chemotherapy, the native recurrence charges had been eight. Some patients with cumbersome T2 lesions near the sphincters should also be thought-about for neoadjuvant chemoradiotherapy to have the ability to enhance sphincter preservation (Table 40-8). Between 60 and 84% of recurrences are seen in the rst 24 months and 90% within 48 months. Endorectal ultrasound in the preoperative staging of rectal tumors: a learning experience. Sequential preoperative uorodeoxyglucose�positron emission tomography evaluation of response to preoperative chemoradiation: a way for determining long-term outcomes of rectal most cancers. A case-controlled examine of 18- uorodeoxyglucose positron emission tomography in the detection of pelvic recurrence in beforehand irradiated rectal most cancers sufferers. Histopathology and prognosis of malignant colorectal polyps treated by endoscopic polypectomy. Lymph node involvement and tumor depth in rectal cancers: an evaluation of 805 patients. Are there patients with stage I rectal carcinoma at risk for failure after abdominoperineal resection Preoperative oral antibiotics reduce septic complications of colon operations: results of prospective, randomized, double-blind scientific examine. Current practices of preoperative bowel preparation among North American colorectal surgeons. Adequacy of 1-cm distal margin after restorative rectal most cancers resection with sharp mesorectal excision and preoperative combined-modality therapy. Anderson Cancer Center expertise with local excision and multimodality therapy for rectal cancer. Transanal endoscopic microsurgery is extra e ective than conventional transanal excision for resection of rectal lots. Ultra-low anterior resection and coloanal pouch reconstruction for carcinoma of the distal rectum. At 5 years, if the patient has had no recurrence, she or he could additionally be followed yearly with clinic visits and may undergo colonoscopy every 3 to 5 years. A methodology of performing abdominoperineal excision for carcinoma of the rectum and the terminal portion of the pelvic colon. Rectal most cancers: the Basingstoke expertise of whole mesorectal excision, 1978�1997. Predictive worth of histology on the invasive margin in the prognosis of early invasive colorectal carcinoma. A research into exterior rectal anatomy: improving affected person selection for radiotherapy for rectal cancer. Total mesorectal excision and native recurrence: a examine of tumour spread within the mesorectum distal to rectal cancer. Lymph node metastases detected in the mesorectum distal to carcinoma of the rectum by the clearing technique: justi cation of whole mesorectal excision. Clinicopathological examine of intrapelvic cancer unfold to the iliac area in decrease rectal adenocarcinoma by serial sectioning. Planes of sharp pelvic dissection for main, domestically superior, or recurrent rectal most cancers. Total mesorectal excision for rectal most cancers: what could be achieved by a national audit A comparison between the remedy of low rectal most cancers in Japan and the Netherlands, focusing on the patterns of local recurrence. Male urinary and sexual capabilities after mesorectal excision alone or in combination with prolonged lateral pelvic lymph node dissection for rectal most cancers. Male and female sexual and urinary operate after whole mesorectal excision with autonomic nerve preservation for carcinoma of the rectum. Costutility analysis of preoperative radiotherapy in patients with rectal cancer undergoing complete mesorectal excision: a research of the Dutch Colorectal Cancer Group. Abdominoperineal resection through whole mesorectal excision and autonomic nerve preservation for low rectal most cancers. Evidence of the oncologic superiority of cylindrical abdominoperineal excision for low rectal cancer. Results after rectal cancer resection with in-continuity partial vaginectomy and total mesorectal excision. Bladder and sexual function following resection for rectal most cancers in a randomized medical trial of laparoscopic versus open approach. Predictors of survival in recurrent rectal cancer after resection and intraoperative radiotherapy.
50 mg cytoxan order visa
Peripheral to the white pulp is the marginal zone that accommodates end arteries arising from the central artery and from peripheral penicilliary arteries treatment 4 sore throat cytoxan 50 mg buy generic on line. Locally produced immunoglobulins enter the marginal zone medicine quiz cytoxan 50 mg discount free shipping, ultimately coursing to the blood stream. Physiology A Spleen receives 250�300 mL of blood per minute, which corresponds to 5% of the cardiac output. A quick (closed) circulation that takes the blood instantly from the arterioles to venules or a slower (open) circulation that takes the blood through the pulp. Functions of the spleen may be usually divided into the following: Erythrocyte quality control and removing of faulty pink cells: is is achieved via pitting and culling. Pitting refers to the elimination of inflexible structures such as Heinz our bodies (denatured intracellular hemoglobulin), Howell-Jolly our bodies, and hemosiderin granules from red cells. Distributed kind: brief splenic artery that divides into long brunches that enter the spleen medially, involving 75% of the medial border. Normally, because the pink cell ages after a life span of approximately 120 days, it loses osmotic balance and membrane integrity, and due to this fact deformability. Normally, about one-third of the platelet mass is pooled within the spleen, and this pool exchanges freely with the circulating platelets that have a life span of about 10 days. With splenomegaly, a large proportion of platelets are sequestered within the spleen (up to 80%) and this, coupled with accelerated platelet destruction within the spleen, accounts for thrombocytopenia. Filtration: Macrophages residing within the splenic parenchyma capture cellular and noncellular materials from blood, including encapsulated micro organism such as pneumococci, and destroy them. Antibody synthesis in the white pulp: In addition to the phagocytosis of antibody-coated cells, the immunologic capabilities of the spleen embrace antibody synthesis (especially immunoglobulin M [IgM]); era of lymphocytes; and manufacturing of tuftsin, opsonins, properdin, and interferon. Foreign antigens which are ltered in the white pulp are offered to lymphoid cells. Isolated splenic damage may be current, or organs in juxtaposition may be concerned; this would come with the stomach, left kidney, left adrenal gland, colon, pancreas, and root of the mesentery. Nonpenetrating or blunt trauma represents an increasing etiologic think about splenic rupture. Diagnostic Studies A lower in serial hematocrit measurements might counsel continued intraperitoneal hemorrhage. Findings on routine stomach lms similar to fractured ribs, elevated left hemidiaphragm, enlarged splenic shadow, medial gastric displacement, and widening of the house between the splenic exure and the preperitoneal fats pad could also be useful. Radiologic classi cation of splenic injury are now well established and may help the clinician establish patients who could be managed nonoperatively (Table 62-1). Spontaneous rupture of the spleen is rare however serious complication of some illnesses. In a review of over 800 spontaneous ruptures, six main etiological groups had been de ned: neoplastic (30. Majority of sufferers had been treated with splenectomy with an total mortality rate of 12%. In a 16-year evaluation of nearly 14,000 colectomies performed at Mayo clinic, the risk of splenic damage requiring a splenectomy or repair was zero. Although restore was tried in 50% of cases, the majority of these patients finally require splenectomy. Bleeding capsular tear or parenchymal laceration 1�3 cm deep with out trabecular vessel involvement. Bleeding subcapsular hematoma or subcapsular hematoma >50% surface area Intraparenchymal hematoma >5 cm in diameter. Laceration involving segmental or hilar vessels producing main (>25% splenic volume) devascularization. Chapter 62 e Spleen 1245 Management Penetrating injury sufferers and hemodynamically unstable blunt trauma patients with hemoperitoneum or peritonitis are treated with laparotomy and certain splenectomy. However, partial splenectomy for trauma antedated this procedure with the rst profitable partial splenectomy for trauma reported by Franciscus Rosetti in 1590. Increasing understanding of the features of the spleen and elevated risk of infection in splenectomized patients have rejuvenated interest in splenic salvage in trauma. Observation that splenic injury could heal itself has also promoted conservative management of splenic injuries, and avoidance of surgical procedure. Increasingly, splenic injuries are managed with close remark and serial hematocrits. Splenic salvage charges with angiographic embolization have been within the order of 90�95%, which doubtless explains the growing sample of its utilization. Although there have been considerations that such nonoperative method would lead to increased need for blood transfusions, this has not been borne out in current literature, even within the nonoperative management of higher grade injuries. Although mycotic aneurysm can be seen within the splenic artery, the bulk are idiopathic. In truth, splenic artery aneurysms have been reported in 14% of sufferers awaiting liver transplant, which may lead to main hemorrhage after transplant. In a contemporary review of 217 splenic aneurysms seen at the Mayo clinic, the mean age at presentation was 62 years, with 79% of the patients being feminine. Over 90% of the patients had been asymptomatic, with solely 5% of patients presenting with a rupture, with a mean size of three. While over 10% of males presented with a rupture, this fee was less than 3% in girls, in large part as a result of bigger aneurysm sizes in men. Such ruptures have been associated with maternal and fetal death charges of 22 and 15%, respectively. Rupture into the colon, abdomen, and gut could take place, however intraperitoneal rupture is by far the commonest presentation. In general, asymptomatic aneurysms greater than 2 cm should be removed if the patient is a 1246 Part X Spleen and Adrenal Cysts Splenic cysts are usually classi ed as primary or secondary (pseudocysts). Some of the splenic tumors can also have a big cystic element to them and are discussed individually in the following text. Primary cysts have an epithelial lining and could be nonparasitic or parasitic (echinococcal). Lesions proximal to the hilus of the spleen may be managed by resection and primary end-to-end anastomosis or proximal and distal ligation with resection of the concerned phase. Distal lesions typically require laparoscopic splenectomy with resection of the concerned splenic artery. Although there was signi cant current progress in treating such aneurysms by endovascular means, with a less than 90% success rate the disadvantages of the endovascular procedures include therapy failures, postprocedural ache, and abscess formation, as nicely as pancreatitis because of occlusion of the pancreatica magna vessel. Echinococcus granulosis, probably the most commonly implicated species, often results in a unilocular cyst composed of an internal germinal layer (endocyst) and an outer laminated layer (ectocyst) surrounded by a brous capsule. Unlike the nonparasitic cysts, these are lled with uid beneath constructive pressure, and likewise contain daughter cysts and infective scolices. Echinococcal cysts are often asymptomatic until they reach a measurement inflicting stress symptoms or become secondarily contaminated or rupture.
Savin Tops. Cytoxan.
- Are there safety concerns?
- Some warts called fig warts, causing abortion, and other uses.
- Dosing considerations for Savin Tops.
- What is Savin Tops?
- How does Savin Tops work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96392
Cytoxan 50 mg buy lowest price
An ultrasonic scalpel or different specialised energy device is used; electrocautery is insu cient to safe hemostasis of these vessels treatment 7 cytoxan 50 mg generic amex. A bougie symptoms 6dpiui purchase 50 mg cytoxan amex, dilator, or comparable space-occupying gadget (some surgeons prefer a exible endoscope) is positioned along the lesser curvature of the abdomen. In the antrum area, the height of the staples used must be longer than within the upper abdomen. Division of the stomach is begun from the area the place devascularization was initiated. Care ought to be taken not to divide the proximal fundus portion of the stomach too close to the gastroesophageal junction and the angle of His. Follow-up for the rst 12 months must be incessantly sufficient to detect issues of long-term stenosis, and occasional dietary issues that may come up. Protein consumption must be encouraged, and liquid protein dietary supplements as properly as dairy-related protein meals often serve as the preliminary largest element of protein consumption. Later, as soon as a bigger quantity of strong meals is consumed, commonplace protein sources within the diet serve to meet protein needs. Vitamin B12 needs supplementation for most patients in the long run, and ranges must be checked beginning a few months after surgical procedure. Once oral drugs are begun, often inside 24 hours, a liquid form of narcotic medicine is most popular initially for ache control. Routine radiographic research on the rst postoperative day is carried out by many surgeons. Patients have a restricted appetite as a result of the anatomic association of the operation. Patient satisfaction with the operation has been reported to be very high as properly. An anatomically related operation, the vertical banded gastroplasty, relied on a shorter lesser curvature tunnel of stomach with a band to constrict out ow. During the1980s, the vertical banded gastroplasty was essentially the most generally carried out bariatric operation within the United States. However, long-term followup confirmed a excessive incidence of patients changing their food plan to accommodate for the restriction, and eating a high-calorie liquid food regimen. Weight regain slowly resulted, and after a decade one institution reported the variety of sufferers with still successful weight loss after vertical banded gastroplasty was beneath 25%. Complications include bleeding, stenosis, and staple line leakage as problems arising soon after surgery, with overall short-term complication incidences reported in the vary of 2�5%. Treatment of postoperative hemorrhage could also be di cult endoscopically, because of the tightness of the lumen of the gastric tube. Operative treatment could additionally be needed if initial Chapter 27 Morbid Obesity and Its Surgical Treatment 557 conservative remedy with transfusions fails or hemodynamic instability happens. Leaks from the staple line are in all probability finest handled initially with operative intervention to restore them. Depending on the circumstances, tissue high quality, degree of peritonitis and soiling, a jejunal feeding tube could additionally be appropriately placed for a secure web site for enteral vitamin. Recurrent leakage may be amenable to endoscopic stent placement as therapy, depending on the lumen of the gastric pouch and the location of the leakage. Balloon endoscopic or uoroscopic dilation is indicated because the initial remedy of selection if feasible. Laparoscopic Roux-en-Y Gastric Bypass Laparoscopic Roux-en-Y gastric bypass is essentially the most frequently carried out bariatric operation within the United States. While there are many variations on the theme, there are particular de ned characteristics and parts of the operation that are frequent to all procedures bearing this name. Wherever possible, mention of frequent variations on every step of the operation will be included. Both arms are normally out to the perimeters for vascular entry, and supported appropriately. Normally a rst-generation cephalosporin will su ce to cover the proximal intestine oras that are potential pathogens in this operation. Pulmonary embolism is doubtless considered one of the main causes of demise after bariatric surgery, and many surgeons use all measures possible to lower its incidence. However, measures prior to surgical procedure often are no much less than foot or leg sequential compression devices or some type of heparin remedy. Many papers have been written on this subject in the literature, and not using a clear consensus. Skin preparation is with a normal chlorhexidine or iodine-based solution, with coverage of the entire abdominal wall up to a degree 2 in above the xyphoid. Instead, utilizing a normal tracheostomy hook to elevate the fascia produces an excellent countertraction of the abdominal wall that allows the Veress needle to penetrate the peritoneal cavity despite the thickness of the abdominal wall. Our most well-liked web site of creation of the pneumoperitoneum is the left upper quadrant, close to the costal margin, where the assistant will have his or her right hand 12-mm trocar port. In tremendous overweight patients, a pneumoperitoneum stress of 18 is often required for adequate visualization. At times, in extremely obese people, the addition of an additional port or two is required. If this proves to be the case, we simply insert an extra port decrease in the midline. Once the omentum is free, is it positioned above the level of the transverse colon, and the transverse colon mesentery then grasped and elevated to assist expose the ligament of Treitz. Once identied, the proximal jejunum is then divided between 30 and 50 cm distal to the ligament. Generally, dividing the bowel on the 50 cm stage provides a proximal finish of the Roux limb that can reach the proximal stomach in even very large sufferers. However, the division of the mesentery must proceed in a direction instantly downward on the mesentery, equally dividing the mesentery between the two segments of divided bowel. Straying to both facet will cause ischemia to one of the bowel segments, requiring additional resection back to viable tissue. Care must be taken to apply slow utility of power in several adjoining factors when dividing the main crossing vessels of the jejunal mesentery. Chapter 27 Morbid Obesity and Its Surgical Treatment 559 but at first the surgeon might want to use an instrument or some marker that helps estimate intestinal size. In this fashion the mesentery of the Roux limb has a continuous bend in a counter-clockwise path as the limb is being measured. Once the suitable length of Roux limb is measured, that time is sutured to the biliopancreatic limb with a single suture on the antimesenteric facet of the Roux limb connecting to the antimesenteric floor of the biliopancreatic limb about 6 cm proximal to its end. Resected items of intestine are both eliminated immediately now or positioned in a specimen bag for later removal, relying on their dimension. We have found that this double- ring method primarily eliminates the occasional concern of stenosis of this distal anastomosis, a complication that may prove deadly. Finally, the mesenteric defect of the enteroenterostomy is closed with a working permanent suture, starting on the base of the mesenteric defect and completing the suture by sutures between the top of the biliopancreatic limb and the side of the Roux limb a number of centimeters beyond the enteroenterostomy. Some surgeons choose to create the enteroenterostomy utilizing a single-stapled method.

Cytoxan 50 mg free shipping
Some instances of chronic pancreatitis are attributed to sphincter of Oddi dysfunction treatment 4 stomach virus order cytoxan 50 mg amex, though rigorous evidence to assist this affiliation can also be lacking medicine 4839 cytoxan 50 mg order line. Traditional theories of the pathogenesis of acute pancreatitis embody the toxic-metabolic or oxidative stress hypotheses, in which regular acinar cell processing and launch of zymogens are disrupted by a poisonous or oxidative stressor, and the ductal obstruction hypothesis that proposes a mechanical position for ductal plugs and stones causing disruption of the integrity of the acinar cell (common in alcoholic and tropical disease). In certain conditions, notably autoimmune illness, pancreatitis might start not within the acinar cell however in the duct cell, triggered by the development of an as-yet-unidenti ed autoantigen on the duct epithelium. Recently, consideration has centered on understanding the mechanism of pancreatic brosis, the central histological characteristic that characterizes the evolution from acute disease to persistent pancreatitis. However, the injury may not utterly resolve after a severe attack, notably if there was signi cant tissue necrosis. A comprehensive mechanistic explanation for pain, typically probably the most debilitating symptom of persistent pancreatitis, additionally remains elusive. An various, and presumably complementary, hypothesis is that the ache represents a neuropathy attributable to repeated in ammatory insults and harm to retroperitoneal sensory nerves. Some sufferers expertise recurrent attacks of reasonable to extreme pain interspersed with periods of relative or full quiescence. In others, the ache may be persistent and lead to signi cant incapacitation and continual disability. During acute exacerbations, the pain may be increased by meals consumption and is frequently related to nausea and vomiting. Weight loss and malnutrition are widespread, because of both decreased consumption in addition to exocrine insu ciency with consequent malabsorption of protein and fat. Jerrold Turner) is usually obvious in patients with classical steatorrhea (loose, bulky bowel movements which might be greasy, sticky, oily, or foul-smelling), but these signs are obscured by narcoticassociated constipation. Endocrine insu ciency usually occurs late in the course of illness, typically after exocrine insu ciency has appeared, and normally not before about 90% of the pancreatic parenchyma has been changed by brosis. Diabetes is extra widespread in sufferers with alcohol-associated persistent calcifying pancreatitis with 80% of these individuals demonstrating endocrine insu ciency inside 10 years of the development of severe exocrine insu ciency. Histologically, pancreatic islets are seen to persist inside areas of in depth brotic replacement of exocrine tissue. Less is understood concerning the natural historical past of nonalcohol-associated continual pancreatitis but the threat of diabetes seems to be decrease. Elevation of liver function exams, particularly serum bilirubin and alkaline phosphatase, may point out the presence of bile duct obstruction. In the early phases of persistent pancreatitis, ductal or parenchymal adjustments could additionally be rather subtle, but because the disease advances, progressive and irreversible changes in organ architecture are readily apparent. Chronic pancreatitis related to toxic-metabolic or genetic risk factors, and idiopathic continual pancreatitis may demonstrate calci cations both focally or scattered all through the organ. In autoimmune pancreatitis, calci cations are almost uniformly absent and the pancreas is often di usely enlarged although a focal mass-forming variant is occasionally encountered. Some of these patients could su er from practical stomach pain problems somewhat than pancreatic illness. Various methods using as much as eleven totally different parenchymal and ductal endosonographic criteria (Table 56-3) to diagnose persistent pancreatitis have been proposed. Functional testing to demonstrate pancreatic exocrine insu ciency is sometimes useful, though from a practical standpoint, the situation is usually clinically obvious. Symptoms of steatorrhea, postprandial gaseous distension, or progressive weight loss despite enough caloric consumption are all suggestive of exocrine insu ciency. Elevation in fasting serum glucose or glycosylated hemoglobin (HgA1c) suggests pancreatic diabetes. Functional analysis (eg, formal oral glucose or arginine-tolerance testing) for pancreatic endocrine insu ciency could also be useful in patients prior to pancreatic resection, significantly if autologous islet transplantation is under consideration. In patients with suspected autoimmune pancreatitis, measurement of serum immunoglobulin G levels, particularly IgG4, is indicated. Occasionally, sufferers are unable to tolerate oral food intake for prolonged periods of time, by which case dietary support by an enteral route that minimizes pancreatic stimulation (eg, via nasojejunal or gastrojejunal tube) or by a parenteral method may be required. Pancreatic enzyme substitute is used to deal with steatorrhea and other signs of exocrine insu ciency. In certain circumstances, medical remedy might alter the depth or frequency of exacerbations of continual pancreatitis. For instance, some sufferers with early, small duct, or minimal change disease appear to bene t from high doses of noncoated enzyme preparations. Noncoated enzyme preparations should be shielded from destruction by gastric acid suppression remedy; trials that instead make the most of enteric-coated delayed release enzyme formulations showed no bene t. Pain, more than some other characteristic, accounts for intractability and general loss of quality of life. While in some patients, the intensity of pain could burnout as the disease reaches its end stage, this natural historical past is very variable and should take years, if it happens in any respect. Pharmacotherapy for pain ought to begin with nonsteroidal anti-in ammatory drugs, but when more powerful agents are wanted, propoxyphene or tramadol could additionally be used prior to escalating to more aggressive pharmacotherapy. Long-acting narcotics supplemented by short-acting narcotic formulations for breakthrough pain could also be extra e ective than short-acting brokers alone. Unfortunately, narcotic dependency is a standard consequence of the use of these agents. Psychosocial helps similar to counseling are essential to profitable longitudinal management of chronic ache. Variable outcomes have been reported with the utilization of long-acting somatostatin analogues. Alternatives such as placement of infusion pumps for intrathecal supply of narcotics have been anecdotally profitable. If short-term relief if obtained, that is adopted by everlasting neurolysis with one hundred pc alcohol injection. Results of celiac plexus block in chronic pancreatitis have been mixed, but transient improvement (typically not more than 6 months) could also be of bene t in chosen patients. Lithotripsy of pancreatic duct stones and pancreatic duct stent placement has been reported in a quantity of small retrospective series. Technical success may be reliably achieved in appropriately selected patients (eg, manageable stone dimension and local density su ciently close to the working end of the scope and with out intervening duct stricture). However, the e ectiveness of endotherapy over time is commonly less than 50% with respect to improvement in ache or reduction in frequency of attacks. Multiple procedures are sometimes needed, recurrence of strictures and stones is frequent, and the substantial fraction of sufferers that fail typically require surgical intervention. Attempts at endoscopic pancreatic duct stone elimination had been unsuccessful, and the patient underwent pancreaticoduodenectomy. Large-Duct Disease Large-duct persistent pancreatitis is characterised by enlargement of the primary pancreatic duct lumen to a diameter exceeding 7�8 mm.
50 mg cytoxan cheap amex
More current software of devascularization procedures by Orozco and colleagues in Mexico has achieved good outcomes with a 10% rebleeding rate medicine 0031 cytoxan 50 mg order. More just lately treatment quincke edema cytoxan 50 mg with amex, most surgeons have approached devascularizations purely from an abdominal approach. Pressures are again measured and the goal is to decrease the gradient between the portal vein and the best atrium to less than 10 mm Hg. Patients are often in the hospital for 1�2 days and the shunt patency should be documented the day after the process with a Doppler ultrasound. While a Doppler ultrasound will document patency, it has not proved to be a sensitive method for documenting stenoses, which requires direct measurement of the strain gradient. Reintervention rates to keep patency were high with uncovered stents, ranging from 40 to 80%, but have fallen to about 20% with lined stents. Most of this encephalopathy seems to be relatively easily managed with lactulose and/or some minimal protein restriction. Splenectomy, gastric and esophageal devascularization, and esophageal transection are the parts of these operations. Extensive devascularization will scale back the danger of bleeding in such sufferers, and this stays the primary indication for this operation. Postoperative administration requires attention to element to minimize the risk of ascites as these sufferers still have portal hypertension. Follow-up endoscopy around 6 months is often helpful to doc if there are any residual varices, deal with them endoscopically at that time, or doc the completeness of the devascularization process. Overall, the bleeding charges can be decreased to less than 20% with this procedure and encephalopathy rates are low. Liver Transplant Liver transplant is the most commonly used operation for sufferers with portal hypertension these days,50�52 and has been the major advance within the treatment of sufferers with advanced liver disease and sequelae of portal hypertension. Patient choice additionally depends on other variables corresponding to comorbid medical situations and a psychosocial suitability for transplant significantly in the alcoholic and different chemical dependency affected person populations. Timing is dictated by these objective standards somewhat than particular person doctor selections in day-today affected person management. Hospital mortality remains at less than 10%, despite transplanting in sicker and sicker sufferers and despite utilizing more marginal organs. Technical features of liver transplant have focused on use of whole organ grafts, partial segmental grafts, residing donor grafts, strategies of caval preservation, different methods of revascularization, and improved strategies for biliary reconstruction. Improvement in methods of immunosuppression, an infection prophylaxis and therapy, patient monitoring to cut back the risk of transplant-related malignancy, and longterm well being maintenance after transplant are ongoing elds of investigation and enchancment. Patients with cirrhosis ought to have a screening endoscopy to assess for varices and initiate remedy if appropriate. Airway protection, acceptable uid resuscitation, sufficient monitoring, and antibiotic prophylaxis are all now standard of care for such sufferers. Transfusion of blood for bleeding, blood merchandise for coagulopathy should be carefully monitored with a goal of under- quite than over-resuscitation. Pharmacologic therapy with intravenous octreotide (50 g/h) will reduce portal pressure and must be initiated on suspicion of a variceal bleed. Early endoscopy, both for prognosis and preliminary banding therapy, is the mainstay of treatment. In ation of the gastric balloon alone, pulled gently up into the gastric fundus, will usually su ce to management bleeding. If that fails to management the bleeding, the esophageal balloon may need to be in ated to 40 mm Hg. Airway protection, careful monitoring, and acceptable uid management and resuscitation are required. Early evaluation and follow-up endoscopy to initiate an elective course of banding is the next step in total affected person administration. Subsequently one or two banding classes will most likely be required to obliterate these varices. A beta-blocker is started with the goal of reducing the heartbeat price by 20% and with the plan to use this for longterm therapy. Overall patient care additionally mandates a full analysis of the affected person at this point. Occlusion happens in over half by 6 months, disseminated intravascular coagulation is triggered by reinfusion of ascites, and an infection is a signi cant risk on this prone population. It is necessary to di erentiate these pulmonary syndromes because remedy is di erent. Ascites e administration of ascites is primarily medical with dietary salt restriction and diuretics (spironolactone and furosemide). As indicated above, refractory ascites is amongst the major scientific signs of end-stage liver illness. A mean pulmonary artery strain of greater than 25 mm Hg with a capillary wedge pressure of less than 15 mm Hg con rms a prognosis of pulmonary arterial hypertension. Pulmonary artery pressures larger than 50 mm Hg are an absolute contraindication to liver transplantation. Undoubtedly the coordinators are those to whom the sufferers flip for help in navigating their method via administration on this advanced eld. Selective trans-splenic decompression of gastroesophageal varices by distal splenorenal shunt. A review of 15 years experience in using sclerotherapy within the control of acute hemorrhage from esophageal varices. A prospective managed trial of sclerotherapy in the lengthy term management of sufferers after esophageal variceal bleeding. Hyperdynamic circulation of liver disease forty years later: pathophysiology and medical penalties. Prediction of the rst variceal hemorrhage in sufferers with cirrhosis of the liver and esophageal varices. Endoscopists play an necessary function diagnostically and in major remedy for managing variceal bleeding. Surgeons play a significant role in liver transplant however may also have a task in shunting good-risk sufferers with refractory variceal bleeding. Pathologists with an interest in liver pathology are important in the accurate diagnosis and staging of disease severity. Critical care physicians and anesthesiologists are important team members when sufferers with portal hypertension have acute occasions and of their perioperative management. Nephrologists, cardiologists, and pulmonologists all play a job within the management of a few of these patients, and in main centers it could be very important have members of all these specialties in the group who perceive the pathophysiologic adjustments of portal hypertension. A meta-analysis of endoscopic variceal ligation for main prophylaxis of esophageal variceal bleeding. Improved patient survival after acute variceal bleeding: a multi-center, cohort examine.
Cytoxan 50 mg buy with amex
Patients with syphilis must abstain from sexual contact until therapy is full symptoms underactive thyroid order 50 mg cytoxan fast delivery. All sexual contacts inside the previous 90 days should be prophylactically treated treatment 002 purchase 50 mg cytoxan visa. Gonorrhea Anorectal infections attributable to the bacterium Neisseria gonorrhoeae are frequent within the male gay inhabitants and frequently accompany different venereal illnesses. Over half of gay males seen in screening clinics have been discovered to be infected, with the rectum being the only website contaminated in about half of cases. Untreated rectal gonorrhea can result in septic arthritis, endocarditis, perihepatitis, and meningitis, in addition to infection of sexual partners. Several medicine (penicillin, tetracycline, ampicillin, and spectinomycin) may be used for treatment, although growing numbers of resistant strains are being recognized. Fecal Incontinence Quality of Life Scale: quality of life instrument for patients with fecal incontinence. Balloon expulsion check facilitates analysis of pelvic oor outlet obstruction due to nonrelaxing puborectalis muscle. Anorectal perform in patients with defecation problems and asymptomatic topics: analysis with defecography. High-resolution three-dimensional endovaginal ultrasonography within the evaluation of pelvic oor anatomy: a preliminary examine. Benign Anorectal Diseases: Diagnosis With Endoanal and Endorectal Ultrasound and New Treatment Options. One hundred circumstances of anal ssure handled with botulin toxin: early and long-term results. Total anal sphincter saving method for stulain-ano; the ligation of intersphincteric stula tract. Outcomes of primary repair of anorectal and rectovaginal stulas utilizing the endorectal development ap. Evaluation of latest anti-infective drugs for the treatment of genital infections because of herpes simplex virus. Dynamic magnetic resonance imaging defecography: a diagnostic various within the assessment of pelvic oor disorders in proctology. Randomized, managed trial of biofeedback with anal manometry, transanal ultrasound, or pelvic oor retraining with digital steering alone within the remedy of delicate to average fecal incontinence. Manometric squeeze strain di erence parallels useful end result after overlapping sphincter reconstruction. Factors associated with percutaneous nerve analysis and everlasting sacral nerve modulation outcome in sufferers with fecal incontinence. Sacral nerve stimulation is extra e ective than optimum medical remedy for extreme fecal incontinence: a randomized, managed examine. Factors associated with failure of the arti cial bowel sphincter: a study of over 50 cases from Cleveland Clinic Florida. Long-term practical outcomes after laparoscopic and open rectopexy for the therapy of rectal prolapse. Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and end result for 109 sufferers. Currently, there are roughly 149,000 circumstances of colorectal cancer identified within the United States every year. Pancolitis is related to both an earlier and an elevated risk for colorectal cancer when compared to left-sided colitis alone. Screening the colon yearly beginning at 10 years after the prognosis with colonoscopy and a number of biopsies in four quadrants every 10 cm from the cecum to the distal rectum is used to predict when a affected person is at risk for growing colorectal cancer. If high-grade dysplasia is detected in any of the biopsies, the patient needs to have a total proctocolectomy. Some practitioners advocate a surgical resection for low-grade dysplasia as well, whereas some are willing to repeat a colonoscopy with multiple biopsies. If low-grade dysplasia is found on the second short-interval colonoscopy, total proctocolectomy is indicated. Genetic threat elements also have been implicated within the development of colorectal most cancers. Extraintestinal manifestations of this genetic defect include desmoid tumors, periampullary masses, osteomas, and medulloblastomas. In 1885, Kraske pioneered the transsacral strategy of rectal resection and anastomosis. Furthermore, he advocated removal of the rectum with a high ligation of the superior hemorrhoidal artery as nicely as excision of the stomach attachments of the rectum and the iliac lymph nodes. Over the following 80 years through the late Eighties, mortality and morbidity for rectal cancer surgery improved markedly in pace with improvements in intra-, peri-, and postoperative care. Unfortunately, there have been few, if any, advancements in oncologic techniques throughout this era. Moreover, Heald described a "zone of downward spread" within the mesorectum that requires complete excision so as to cut back local recurrence. Finally, native excision of small rectal cancers has been used for a a hundred years in chosen sufferers. More recently, native excision is being mixed with neoadjuvant and adjuvant chemoradiotherapy to maximize local management with a minimally invasive approach. Despite the name, these cancers arise from adenomas and should account for 5% of all colorectal malignancies. In this autosomal dominant syndrome, cancers happen more often on the right side of the colon. Family members ought to be screened initially at age 20 years with colonoscopy for the presence of polyps or colon cancer. If a polyp or most cancers is detected, a complete abdominal colectomy with an ileorectal anastomosis is recommended. Urine cytology to rule out dysplastic cells within the genitourinary tract (which is at risk for transitional cell carcinoma) is really helpful. Any a ected lady who has nished childbearing and requires a colectomy should give robust consideration to a prophylactic complete abdominal hysterectomy and bilateral salpingo-oophorectomy. Dietary fat, particularly red-meat fat, have been implicated as a threat factor for colon and rectal most cancers. In the past few decades, several research have linked alcohol consumption and tobacco use with an increased threat of colorectal neoplasia. Moreover, there appears to be a synergistic e ect with a good higher increased danger of adenomatous polyps in people who are both people who smoke and drinkers. Subsequently, mutations resulting in inactivation of tumor suppressor genes, such as p53, allow for progression to cancer. Most adenomas stay benign; nonetheless, histologic sort, polyp size, and proof of dysplasia are associated with transformation. Tubular adenomas often form a stalk, whereas villous adenomas have a broad base. Only 1% of polyps lower than 1 cm in diameter show evidence of malignant transformation, whereas 50% of polyps greater than 2 cm in diameter harbor areas of carcinoma. Clinically, it is essential to diagnose the type, dimension, and number of polyps to risk-stratify sufferers for remedy and future surveillance.
Real Experiences: Customer Reviews on Cytoxan
Ilja, 26 years: In addition, the gravid uterus can displace the stomach viscera, shifting the placement of the appendix from the proper lower quadrant. Occasional suture ligatures may be needed to stop brisk arterial or venous bleeding. Care must be taken not to divide the proximal fundus portion of the abdomen too close to the gastroesophageal junction and the angle of His.
Sugut, 38 years: In creating nations the height incidence is in males in the 40- to 60-year age group that account for as much as 90%. It is essential to observe, nonetheless, that small bowel radiography may not identify all such lesions. Peptic ulceration of the third or fourth parts of the duodenum is distinctly uncommon; incidence of ulcers in these areas raises the potential of gastrinoma.
Faesul, 57 years: Continence and stool frequency was acceptable, and the patients might evacuate via the conventional route. Additional modi ers are used to re ect the strategy of stage dedication (p for pathology, c for scientific, u for ultrasound), and y to indicate a standing after neoadjuvant treatment. Frequently, the descending department of the left gastric artery is in shut proximity to the location where the hepatic/gallbladder branches take o toward the liver in the gastrohepatic (lesser) omentum.
8 of 10 - Review by D. Enzo
Votes: 262 votes
Total customer reviews: 262
