Gemfibrozil dosages: 300 mg
Gemfibrozil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
300 mg gemfibrozil discount
Plain radiograph of the best forearm shows no evi dence of fracture cholesterol test glasgow gemfibrozil 300 mg buy line, fuel cholesterol test walgreens 300 mg gemfibrozil discount with amex, or foreign physique. Medical history is critical for liver transplantation 6 months ago for major biliary cirrhosis; she was sero unfavorable for cytomegalovirus and Epstein-Barr virus, and her donor was positive for both. She describes the rash as irritating however not painful or related to any systemic symptoms. She has had a similar rash roughly four times over the previous yr in the identical space. She stories that when the rash has occurred before, the lesions final roughly 6 days, then crust over and resolve. On a number of events, she observed a extreme headache lasting 2 to 3 days when she had the rash. She is married, and her husband has not had Self-Assessment Test any comparable signs. The rash, located at the mid-lower sacral area lateral to the gluteal crease, is proven. Three days ago, she ate almond butter from a manufacturer that posted a voluntary recall of the product because of contamination with On bodily examination, temperature is 37. He stories declining influenza immunization supplied within the autumn months because his sister advised him that a good friend developed a neuro logic sickness after receiving the vaccine. Med ical history is significant for asthma, and his solely medica tion is inhaled albuterol as wanted. Which of the next is the most appropriate influenza prophylaxis routine to recommend to this patient Her household notes that yesterday she seemed confused and had bother getting dressed. Sputum Gram stain reveals 2+ leukocytes and 3+ gram-negative rods; sputum culture is pending. In addition to appropriate empiric antibiotics, which of the following further interventions is most likely to enhance outcomes His only med ication is once-daily mixture tenofovir-emtricit abine-cobicistat-elvitegravir initiated last month. Laboratory research are vital for a rise in his serum creatinine from his pretreatment baseline of 1. Urinalysis is dipstick unfavorable for blood or protein, and microscopic examination shows no cells or casts. She was in a motorized vehicle accident 7 days in the past and has required 122 Item 65 A 37-year-old man is hospitalized for diabetic foot infection with sepsis of the proper lower extremity. Medical history is significant for kind 2 diabetes mellitus with a baseline creatinine of J. Result of stool polymerase chain reaction assay is positive for Closlridium difficile toxin. She has no historical past oftravel outdoors the United States and no identified infectious exposures. Laboratory studies show a standard metabolic profile, kidney and liver operate. The cerebrospinal fluid is obvious with a leukocyte rely of 1/�L (1 x 10 6 /L and an erythrocyte depend of 0/�L. Item 67 A 32-year-old man is evaluated in the emergency depart ment for a 2-day historical past of fever. He is employed as an international emergency aid worker and recently returned to the United States after an prolonged abroad Item 68 A 32-year-old man is evaluated in the emergency depart ment for a extreme occipital headache. He signifies that he had a reddish pores and skin rash positioned across his chest and higher stomach that first appeared a quantity of days after onset of his fevers and different symptoms and commenced to fade a number of days ago: the rash was current for roughly l week. Which of the following research is most probably to confirm the prognosis on this patient He stepped on a metallic object that punctured via his leather work boots into the plantar side of his foot. Medical historical past is important only for a fracture of the fourth and fifth metatarsal bones ofthe proper foot 27 years ago treated with an inside fix ation plate. Item sixty nine (B) Mycobacterium gordonae (C) Mycobacterium kansasii (D) Mycobacterium marinum Which of the following is probably the most applicable diagnostic test to carry out subsequent Five days in the past he underwent alternative of a ventriculoperitoneal shunt used to manage congenital hydrocephalus. The procedure was unremarkable, and he did nicely postoperatively until the speedy onset of confusion and fever over the past several hours. Laboratory analysis of the cerebrospinal fluid exhibits a leukocyte count of 4660/�L (4660 x 106/L) with neutrophilic predominance, glucose stage of 15 mg/dL (0. Item 71 Cl Which of the following is essentially the most acceptable empiric antibiotic remedy She stories that she often visits a local spa that makes use of whirlpool footbaths during her pedicure procedures: she always shaves her legs with a razor before these visits. Several mildly tender, erythematous nodules and papules are famous over the dis tal decrease extremities bilaterally; a quantity of lesions appear furuncular with associated ulceration. He has sex with different males and is cautious about choice of companions: because of this, he expresses disbelief on the prognosis. Item seventy two Self-Assessment Test Which of the following is the most appropriate next step in administration She was admitted for management of accidents sustained in a motorcar accident and has undergone multiple orthopedic sur gical procedures. Urinalysis reveals 25 to 30 leukocytes/hpf" and greater than 10s colony-forming units of yeast identified as Can Which of the following is the most acceptable administration Which of the following is essentially the most applicable empiric antibiotic therapy for this affected person He notes that the cough is min imally productive of a small amount of whitish sputum. Medical history is notable only for cellulitis 2 months in the past handled with a brief course of cephalexin. Pulmonary examination reveals decreased breath sounds at the right lung base with no wheezes, crackles, or rhonchi auscultated. Item seventy five Item 74 A 46-year-old man is diagnosed with methicillin-sensi tive Staphylococcus aureus osteomyelitis of the L2 and L3 vertebrae during a latest hospitalization. Which of the following checks ought to be completed weekly in monitoring this affected person One week in the past, he presented to his internist with a pores and skin eruption on his stomach, which was recognized as erythema migrans. Laboratory stuilies: 125 mg/ell (1250 mg/L Haptoglobin 45% H matocrit 2300/�L (2.
Order 300 mg gemfibrozil
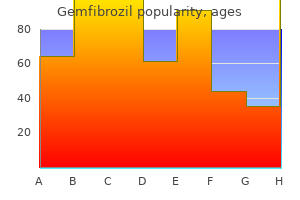
The outcomes of spirometry are extremely depending on technique and patient effort; due to this fact cholesterol chart 2015 gemfibrozil 300 mg purchase otc, patients must be rigorously instructed in the correct technique prior to cholesterol ratio 2.8 good or bad purchase gemfibrozil 300 mg fast delivery testing. Proper method consists of the affected person sitting upright with the top erect and the mouthpiece held tightly between the lips. Measurements ought to be repeated to ensure reproducibility; the two largest values inside a hundred and fifty mL of each other should be used. Normal reference values for spirometry are depending on age, gender, top, and race. Bronchial Challenge Testing In patients with medical symptoms suggestive of bronchospas tic illness (such as cough or unexplained dyspnea) but with normal spirometry, bronchial problem testing could also be diag nostically useful. Because bronchial problem testing might induce extreme bronchospasm, it ought to solely be performed in a controlled setting similar to a pulmonary perform testing laboratory. Methacholine is a generally used agent that induces cholinergic bronchospasm at low concentrations in sufferers with asthma. Lung Volumes Lung quantity testing instantly and not directly measures the static amount of air within the lungs and could be helpful in the diagnostic evaluation of dyspnea and irregular spirometry results. The parts that are immediately measurable by plethysmography are the functional residual capability (air within the lungs after a 1 � Bronchial challenge testing with a managed stimulus is useful in patients with dyspnea or cough of uncertain trigger when spirometry outcomes are regular. Top left panel: Flow-volume loop demonstrating normal spirometry, with comparable most inspiratory and expiratory flows; no important change is seen after Volume lnspiratory Flow Volume bronchodilator administration. Top right panel: Flow-volume loop demonstrating asthma, with a discount in peak expiratory move and concave curvature for the expiratory limb whereas the inspiratory limb remains regular; improvement is seen in expiratory flows (particularly the increase in peak flow) after bronchodilator administration. Bottom proper panel: Flow-volume loop demonstrating fixed obstruction/tracheal stenosis, with flattening of the height inspiratory and expiratory flows. Simple pulse oximetry and oxygen desatura tion studies performed at rest and with exertion assess the necessity for oxygen supplementation. This rela tively easy maneuver quantifies exercise tolerance, deter mines efficient interventions, and helps predict morbidity and mortality. Pulse Oximetry Pulse oximetry is a noninvasive measurement of arterial hemoglobin saturation. Pulse oximeters have two mild emitting diodes and a photodetector that measures the pul satile fraction of hemoglobin and algorithmically estimates the arterial hemoglobin saturation. In basic, resting oxy gen saturation lower than or equal to 95% or a desaturation with exercise larger than or equal to 5% is taken into account abnormal. In sufferers with excessive ranges of automobile boxyhemoglobin, as seen in carbon monoxide poisoning, pulse oximetry will present false-negative results. If the pres ence of carboxyhemoglobin is suspected, co-oximetry is the popular take a look at to measure oxyhemoglobin. It is therefore usually the primary diagnostic check carried out when evaluating any symptoms potentially defined by pathology to any of these buildings. The price and risks to the affected person, such as subsequent penalties of radiation exposure (Table 1), are decrease com pared with different chest imaging studies. Posteroanterior and lateral chest radiographs displaying normal cardiopulmonary and skeletal structures. Comparison of Radiation Exposure of Chest Imaging Techniques Imaging Modality Equivalent Daytime Radiation 10 days three years 89 days four. The decrease dose of radiation decreases the radiation to patients and is as efficient in imaging lung nodules and lung parenchyma owing to the excessive inherent contrast between lung tissue and air. Computed Tomography 1:iberoptic bronchoscopy is an endoscopic approach that enables f<lr the visualization or the tracheobronchial lumen:me sampling or suspected areas or illness. It can be used for staging the cancer (by deter mining the presence or absence of metastatic disease), moni toring response to therapies (not solely by assessing for a lower in size but additionally for a decrease in metabolic activity), and surveillance for recurrence. The most typical inclicat ions for a bronchoscopy are (t) analysis of new respiratory symptoms related to airway pathology (for example. P,llicnts may have aclvcre effects rrom topicJ I anesthctics and systemic sedatives. J latest rnyoc,irdial inrarction or who requires excessive quantities ofsupplcmemal oxygen. An electromagnetic steerage system on the bronchoscope is then used to create a map of the airways and guide the doctor to the world of interest. Indication Hemoptysis Common Indications for Diagnostic Bronchoscopy Comments Patients with energetic hemoptysis with out an obvious rationalization warrant an airway inspection via bronchoscopy and chest imaging. Bronchoscopy could also be useful in localizing an active bleeding supply in addition to for treatment of endobronchial abnormalities causing bleeding. Bronchoscopy can identify the placement of airway obstruction and can also deal with the underlying trigger (for example, removal of a overseas physique or balloon dilation of a stricture). These sufferers generally have opportunistic infections together with Pneumocystis jivorecii pneumonia and fungal infections. Bronchoscopic biopsy of lung nodules and much coupled with lymph node aspiration might help diagnose and stage lung cancers. Stridor or localized wheeze Pulmonary infections Diagnosis and/or staging of bronchogenic carcinoma Diagnosis of pulmonary metastases Evaluation of a pulmonary nodule Persistent pulmonary infiltrate Mucus plugging Foreign-body aspiration Diffuse parenchymal lung disease Diagnosis of metastatic illness may be made by bronchoscopy and biopsy in sufferers presenting with new pulmonary nodules within the setting of a identified major most cancers. Diagnostic specimens may be obtained via bronchoscopic biopsy for tissue prognosis. Patients with a persistent pulmonary infiltrate could profit from bronchoscopy to diagnose or exclude noninfectious causes of pulmonary infiltrates, similar to eosinophilic lung illness, cryptogenic organizing pneumonia, and most cancers. When mucus plugging is extreme sufficient to cause atelectasis and intrude with oxygenation or air flow, bronchoscopy might evacuate the mucus plug. Bronchoscopy is the intervention of choice to extract foreign our bodies wedged in airways. Surgical lung biopsy is the diagnostic technique of alternative for many patients with diffuse parenchymal/interstitial lung illnesses. However, chosen illnesses, together with sarcoidosis, are diagnosed with a excessive diploma of accuracy through bronchoscopic strategies, which may obviate the need for a extra invasive surgical biopsy. The ultrasound-tipped bronchoscope can identify mediastinal lymph nodes and improve the yield or a transbronchial needle aspiration by allowing direct visuali zation of the needle entering the lymph node. Peripheral bron choscopic ultrasound methods also can aid in the success ful biopsy of any lesion adjoining to an airway. I:) 6 � Fiberoptic bronchoscopy is an endoscopic approach that allows for the visualization of the tracheobronchial lumen and sampling of suspected areas of disease, together with the endobronchial mucosa, lung parenchyma, and accessible lymph nodes. Differentiation of bronchial asthma subtypes may allow therapeutic approaches to be tailored for the person affected person, leading to maximal remedy efficacy with minimal adverse effects. Commonly noticed clinical syndromes of bronchial asthma in addition to confounding factors that worsen underlying asthma shall be discussed on this chapter. Epidemiology and Natural History Asthma impacts approximately 8% of the population in the United States. Allergic bronchial asthma is strongly associated with a private or family history of allergic reactions or atopy (maternal bronchial asthma in particular), maternal smoking while pregnant, and exposure to environmental tobacco smoke in childhood. Children with allergic bronchial asthma are generally recognized Airways Disease throughout preschool years, and many have gentle signs that resolve. However, some people with childhood allergic bronchial asthma progress to chronic airflow obstruction with increas ingly extreme signs that persist into maturity. Although the trigger is unclear, this worsening of bronchial asthma into maturity is likely associated to environmental stimuli similar to viral infec tions, office exposures, or exposure to tobacco smoke (first-hand or second-hand) in addition to individual predisposi tion (for instance, family historical past, antioxidant activity in the lung).
300 mg gemfibrozil cheap visa
Liver chemistry test abnormalities have been reported with continual tolvaptan remedy; subsequently cholesterol test limerick buy gemfibrozil 300 mg with mastercard, using this drug should be limited to less than 1 to 2 months cholesterol to hdl ratio gemfibrozil 300 mg without prescription, with close labora tory monitoring. Considerably much less widespread than hyponatremia, hyper natremia is related to mortality charges of approximately 40% to 60%. Elderly people with lowered thirst and/or diminished entry to fluids are on the highest risk of creating hypernatremia. More generally, hypernatremia may develop following the Joss of free water through renal or extrarenal routes. Insensible losses of water because of evaporation from the pores and skin or respiratory tract could increase within the setting of fever, exercise. Osmotic diarrhea and viral gastroenteritides typically generate hypo-osmotic stools, leading to important free water loss and hypernatremia. Common causes of renal water loss embody osmotic diu resis secondary to hyperglycemia, post-obstructive diuresis, or medication (contrast, mannitol). H 2 0 Deficit Correction of Hypernatremia Central diabetes insipidus Autoimmune hypophysitis (idiopathic)� Malignancy (metastatic or primary)� Neurosurgery� Infiltration (sarcoidosis, histiocytosis X, lymphocytic hypophysitis, granulomatosis with polyangiitis [formerly often known as Wegener granulomatosis], lgG4-related disease)" Trauma Following correction of supraventricular tachycardia Hypoxic encephalopathy Anorexia nervosa Sheehan syndrome Familial Nephrogenic diabetes insipidus Lithium� Other medicines (demeclocycline, cidofovir, foscarnet, didanosine, amphotericin B, ifosfamide, ofloxacin)� Electrolyte issues (hypercalcemia, hypokalemia)� Urinary tract obstruction Sickle cell nephropathy Amyloidosis Sjogren syndrome Nephronophthisis Cystinosis aMost widespread causes. Gestational diabetes insipid us (placental "vasopressinase") 1 1 fluid intake and daily urine output can additionally be required. The appropriate renal response to hypernatremia and a plasma osmolality >295 mOsm/kg Hp is the excretion of low volumes (<500 mL/24 h) of maximally concentrated urine (>800 mOsm/kg Hp). Most sufferers with hypernatremia and polyuria have a predominant water diuresis with hypotonic urine. However, those who have an osmotic diuresis as a reason for hyperna tremia will reveal extreme excretion of sodium chlo journey, glucose, and/or urea. The water deficit must be corrected over 48 to 72 hours to avoid neurologic compromise. Depending on the blood strain or medical quantity standing, preliminary remedy with hypotonic saline options (1/ four or half of normal saline) could additionally be appropriate; plasma glucose must be monitored in sufferers treated with giant volumes of 5% dextrose in water. Calculation of urinary electrolyte-free water clearance is helpful to estimate day by day, ongoing lack of free water in patients with nephrogenic or central diabetes insipidus. Disorders of Serum Potassium Hypokalemia is defined as a serum potassium concentration <3. Symptoms range from generalized weakness and malaise to paralysis, relying on the serum potassium degree. Hypokalemia can happen from transcellular shift of potas sium or from a decrease in total physique potassium by way of decreased consumption, renal loss. The blood strain (including exami nation for orthostasis) and volume status ought to be assessed. Pseudohypokalemia, a laboratory artifact brought on by uptake rapidity of the lower. In patients with heart conditions, delicate to average hypokalemia increases the chance of cardiac. Abrupt development of hypokalemia suggests a tran sient shift of potassium from the extracellular compartment into cells. Medications generally end in intracellular shifts, together with sympathomimetic brokers (epinephrine, decongestants. Systemic alkalosis (respiratory, metabolic) may be associated with acute hypokalemia. Hypokalemic periodic paralysis is a rare famil ial or acquired disorder characterised by flaccid generalized weak point from a sudden intracellular potassium shift pre cipitated by strenuous exercise or a high-carbohydrate meal. Hypokalemia from decreased total body potassium can be the results of extrarenal or renal losses. Because the child neys can cut back urine potassium excretion to <20 mEq/24 h (20 mmol/24 h), hypokalernia from inadequate consumption is unusual. Assessment of urine potassium excretion is important to set up renal potassium wasting. Conversely, urine potassium loss <20 mEq/24 h (20 rnmol/24 h) suggests mobile shift. Urine potassium loss can be caused by enhanced sodium delivery and urine flow to the amassing duct and increased mineralocorticoid exercise (Table 9). Blood stress measure ment might help outline the cause: sufferers with increased min eralocorticoid activity have evidence of volume enlargement with elevated blood pressure. Patients with hypokalemia because of increased distal sodium delivery can have findings of quantity depletion and low or normal blood strain. Magnesium depletion ought to be corrected because it could cause and maintain renal potassium loss. Signs and symp toms are associated to adverse effects of serum potassium on skeletal and cardiac muscle cell membranes. Cl Increased Urine Flow or Sodium Delivery to Distal Nephron Diuretics: loop diuretics; thiazides; carbonic anhydrase inhibitors Antibiotics: high-dose penicillin Osmotic diuresis: diabetes mellitus; mannitol Saline diuresis Renal tubular acidosis Gitelman syndrome Bartter syndrome Increased Mineralocorticoid Activity Exogenous mineralocorticoid Primary hyperaldosteronism: adrenal adenoma; bilateral adrenal hyperplasia; glucocorticoid-remediable aldosteronism Congenital adrenal hyperplasia: 17-o:-hydroxylase deficiency; 11-hydroxylase deficiency Secondary hyperaldosteronism: renin-secreting tumor; renovascular illness Liddle syndrome 11-hydroxysteroid dehydrogenase deficiency: congenital; acquired (licorice, carbenoxolone) Cushing syndrome Evaluation Initial analysis of hyperkalemia begins with the historical past. Laboratory studies must be targeted toward the analysis instructed by the his tory and physical examination. Hyperkalemia may result from increased potassium intake, decreased urine potassium excretion. Excessive intake and extracellular shift are uncommon as the solely real causes or hyperkalemia. Pseudohyperkalemia occurs with a false rise in potassium values from mobile launch of potassium dwing venipuncture because of hernolysis or extended tourniquet use. Pseudohyperkalemia can be dominated out by checking serum and plasma potassium ranges simultaneously, with the plasma stage being normal. Major underlying causes of persistent hyperkalemia are issues during which urine potassium excretion is impaired. Medications commonly associated with hyperkalemia from impaired aldosterone activity embrace potassium-sparing diuretics. Calcium infusion is contraindicated in digoxin toxicity because it may possibly worsen the myocardial effects. Shifting of potassium from extracellular to intracellular is completed both with insulin or with high-dose inhaled -adrenergic agonists. Insulin is given as 10 models intravenously with 50 mL of 50% dextrose; this acts in 10 to 20 minutes, and duration is four to 6 hours. The onset of motion of -adrenergic agonists is three to 5 minutes and lasts for 1 to 4 hours. Sodium bicarbonate may be used to promote intracellular shift of potassium within the setting of metabolic acidosis. Potassium excretion could be increased with using loop diuretics in combination with saline infusion to guarantee delivery of sodium to the distal nephron with normal kidney perform. Long-term remedy of hyperkalemia should be directed at correcting the underlying trigger along with initiating a low-potassium diet and discontinuing hyperkalemia-causing medicines. Spurious hypophosphatemia can be caused by interference of paraproteins with the phos phate assay.
Generic gemfibrozil 300 mg online
Fertility increases after kidney transplantation cholesterol ratio british heart foundation 300 mg gemfibrozil discount free shipping, although fertility rates remain lower and pregnancy compli cations greater compared with the general population cholesterol medication without joint pain order gemfibrozil 300 mg without prescription. Transplant recipients are recommended to wait a minimum of 1 to 2 years after transplant earlier than trying to conceive. There 1s no consensus concerning initiation of remedy; nevertheless, most specialists provoke remedy at blood pressures >150-160/100-110 mm Hg. Glucocorticoids, cyclo sporine, tacrolimus, and azathioprine have been used dur ing being pregnant. Potential issues from glucocorticoids include infection and adrenal insufficiency. Criteria for the Diagnosis of Chronic Kidney Disease� Marker of kidney injury Moderately increased albuminuria or severely increased albuminuria b Abnormal urine sediment (such as hematuria) Electrolyte or different abnormalities caused by tubular dysfunction Histologic abnormalities of the kidney Structural kidney abnormalities detected by imaging Previous kidney transplantation � Women with persistent kidney illness require precon ception counseling due to the larger threat of preg nancy issues corresponding to preeclampsia and declin ing kidney perform when the prepregnancy serum creatinine exceeds 1. Because Persistent albuminuria classes Description and vary A1 Normal to mildly elevated <30 mg/g A2 Moderately increased 30-300 mg/g A3 Severely increased >300 mg/g 1. G1 Cl> Normal or excessive Mildly decreased Mildly to reasonably decreased Moderately to severely decreased Severely decreased Kidney failure. Prognosis of persistent kidney disease by glomerular filtration rate and albuminuria class. Establishing the cause is essential for guiding remedy and estimating prognosis. The trigger may have necessary implications with regard to outcomes and management after kidney transplantation. However, in some studies there was a decrease threat of a composite kidney failure finish point in patients with elevated proteinuria; therefore, some specialists still suggest a lower blood pressure goal of <130/80 mm Hg in sufferers with heavy proteinuria. As kidney operate declines, the conventional homeostasis of cal cium and phosphorus ranges by the kidney turns into compro mised, leading to alterations in bone mineralization. Progressive decline in 1,25-dihydroxy vitamin D levels ends in reduced intestinal calcium absorption, and hyperphos phatemia promotes precipitation of calcium and phosphorus in extraskeletal tissues, leading to hypocalcemia. It is related to an increased number and activity of osteoblasts and osteoclasts and expansion of osteoid surfaces, resulting in an elevated risk of fracture. Classic skeletal modifications on radiograph could embody subperiosteal resorption of bone, most prominently on the phalanges of the palms. Histopathologic abnormalities include decreased osteoclast exercise with an increase in osteoid, leading to an elevated threat of fracture. It is essential to rule out adynamic bone disease previous to bispho sphonate remedy as a result of these medicine can cause and/or worsen this disease by inhibiting osteoclast exercise. Osteomalacia Increased intestinal calcium absorption Decreased calcium excretion t Serum Ca++ Osteomalacia is characterized by decreased mineralization of osteoid at sites of bone turnover. The commonest signs of osteomalacia embrace bone ache and tenderness and elevated threat of fracture. Metabolic Acidosis � the first step in managing secondary hyperparathy roidism is to appropriate 25-hydroxy vitamin D deficiency and normalize the serum calcium and phosphorus, thus eliminating the stimulus for parathyroid hormone secretion. However, excessive alkali supplementation above the traditional vary may also be associated with opposed out comes with metabolic alkalosis. The most typical alkali for mulations prescribed are sodium bicarbonate and sodium citrate (citrate is metabolized to bicarbonate). In the Modification of Diet in Renal Disease examine, no definitive benefit was seen in renal outcomes in sufferers randomly assigned to the low protein (0. Small research recommend that low protein diets might delay the onset of symptomatic uremia and the necessity for renal alternative therapy in chosen sufferers. Protein Restriction Special Considerations Imaging Protein-restricted diets have been shown to slow the development of kidney disease in animal models. Eff011s to lower mortality in this weak population are therefore primarily centered upon preventing cardiovascular and infectious issues. First, the best medical outcomes happen with "preemptive transplants," during which patients receive the transplant previous to dialysis. Peritoneal Dialysis See Vascular Access for data on vascular entry in sufferers present process hemodialysis. Recent knowledge suggest that more frequent and/or longer dialysis ses sions supplied in-center or at home could present some well being benefits, including better control of volume and electrolytes (particularly phosphorus). Patients receiving extra frequent and/or longer dialysis are additionally usually able to liberalize their diet with regard to potassium, phosphorus, and fluid consumption. Because longer and/or extra frequent hemodialysis has not yet been demonstrated to lower mortality in a randomized managed trial, the choice of hemodialysis modality and web site of dialysis must incorporate affected person desire and other fac tors, together with availability of enough residence sources and support. In patients with minimal residual kidney function who with draw from dialysis, most die within 2 weeks. The ready listing for transplants varies markedly by area within the United States. Because the most effective outcomes happen in patients who obtain a preemptive transplant from a residing donor, early referral for transplant analysis to identify appropriate residing donors is essential. If no dwelling donor is out there, early transplant itemizing is crucial to decrease waiting time for a transplant. Patients and donors are carefully screened for potential issues which will affect the protection and/or consequence of the trans plant, together with the presence of active malignancy, coronary ischemia, or lively infection, and to ensure that there are adequate social helps and financial resources obtainable. Patients are normally managed by transplant nephrologists for a minimal of the primary three to 6 months posttransplant and subse quently co-managed with general nephrologists and/or internists, particularly for comorbidities. In the primary month, the most typical infectious problems are wound infections and urinary tract infections. Patients with kidney transplants must obtain immunosup pressive drugs to prevent their immune system from rejecting the kidney allograft. Doses are typically highest immediately after transplant and are tapered gradually over several months to minimize toxicities related to these medications while maintaining sufficient immunosuppression. The most commonly used immunosuppressants in the instant posttransplant interval for immunosuppression induction are anti-T cell and interleukin-2 receptor blocking antibodies. The most commonly prescribed medicines for persistent maintenance immunosuppression embody calcineu rin inhibitors (tacrolimus or cyclosporine), antimetabolites (mycophenolate mofetil or azathioprine), and glucocorticoids. Similar to other sufferers receiving strongly immunosuppressive drugs, kidney transplant recipients must also obtain prophylaxis in opposition to Pneumocystis jirouecii pneumonia. Immunosuppression of kidney transplant recipients increases the incidence and progression of several kinds of malignancies. Therefore, transplant recipients must be carefully screened for skin cancer and educated on the importance of safety from ultraviolet radiation. Because a quantity of different kinds of most cancers are also extra prevalent and/or have worse outcomes in kidney transplant recipients, it is necessary to screen potential kidney recipients and donors for the presence of lively malignancy previous to transplant. Cl Acute Kidney Injury Because cardiovascular disease is the most typical cause of demise in kidney transplant recipients, aggressive management of cardiac threat components is warranted (See Complications and Management, Cardiovascular Disease). Immunosuppressive drugs, together with calcineurin inhibitors, sirolimus, and glucocorticoids, contribute to dyslipidemia. Although medical research on the efficacy of statins in preventing cardiovascular mortality have yielded conflicting results, a large proportion of kidney transplant recipients obtain these medications. Cyclosporine increases serum ranges of statins; therefore, clinicians ought to think about lowering the dose of statins in sufferers taking cyclosporine. Bone Disease Kidney transplant recipients are at elevated risk of bone dis ease as a end result of several factors, together with secondary or tertiary hyperparathyroidism, unwanted effects of immunosuppressive medi cations, and high prevalence of vitamin D deficiency.
Diseases
- Spongy degeneration of central nervous system
- Tufted angioma
- Fibromuscular dysplasia
- Hereditary hearing loss
- Sensory radicular neuropathy recessive form
- Chromosome 18, trisomy 18p
- Chromosome 15q, trisomy
- 17-beta-hydroxysteroid dehydrogenase deficiency, rare (NIH)
300 mg gemfibrozil purchase with mastercard
Optic coherence tomography is being increasingly used to verify optic nerve injury; this testing makes use of near-infrared gentle to quantify the thickness of the retinal nerve fiber layer in the optic disc and the thickness of the macula worst high cholesterol foods gemfibrozil 300 mg online buy cheap. Knowledge of the other potential diagnoses within the differ ential and their distinguishing options may help cut back misdi agnoses and inappropriate referrals definition of cholesterol buy gemfibrozil 300 mg otc. Some sufferers with a relapsing-remitting course will continue on this method and eventually plateau at a constant stage of disability. However, some will transition to a secondary progres� sive course (red fine), by which incapacity accrues over time with out clear relapsing or remitting occasions. Eventually, nonetheless, recov ery diminishes and permanent disability can accumulate. In roughly 50% to 60% of sufferers with an initial relaps ing-remitting course, relapses turn out to be rare or cease fully after a median of 10 to 15 years, however neurologic incapacity continues to accrue in a slowly progressive manner. Although this subtype usually presents later in life (fifth or sixth decade), fast incapacity accumulation can occur. Although early research of the pure history of the illness sort had implicated sex and age at onset as predictors of rapid progression, current studies have solely supported early incapacity accrual as a predictor of long-term progression rates. The diagnosis, prognosis, and treatment of radio logically isolated syndrome are controversial and the subjects of ongoing analysis. Maintenance of an 61 Multiple Sclerosis active healthy life-style and muscular fitness can mitigate disability to some extent and preserve acceptable muscle tone. Physical therapy and residential train programs are use ful on this regard, especially after a clinical relapse. In sufferers with significant Uhthoff phenomenon, minimization of discomforting signs may be achieved with strategies aimed at avoiding heat publicity or cooling the body. However, the danger of relapse in the first three months after supply is significantly increased. Frequent glucocorticoid therapy must be prevented because it locations patients at risk tor the long-term antagonistic erfects of these drugs. Relapses which are refractory to glucocorticoid therapy could reply to rescue therapy with plasmapheresis. Choosing an appropriate remedy from these choices depends on patient tolerability, threat stratification, and disease exercise. Medication Interferon beta-1 a (three formulations) and interferon beta1 b (two formulations) Glatiramer acetate therapy failure, or tips on how to decide the order in which medi cations ought to be launched. Generally, most physicians rec ommend self-injection medications (one of the interferon beta preparations or glatiramer acetate) as first-line agents, given their favorable danger profiles. The interferon beta preparations (beta-la and beta-lb) use an immunomodulatory cytokine that shifts immune responses away from autoimmunity and increases the integ rity of the blood-brain barrier. Head-to-head studies have shown common equivalence for most of the interferons, although extra fre quent administration resulted in barely elevated efficacy of one or the opposite in some research. Glatiramer acetate, a copolymer of 4 amino acids, is run every day by subcutaneous injection. This medica tion probably has multiple mechanisms of action that end in immunomodulation. Glatiramer acetate and high-dose inter feron betas exhibit similar reductions in relapse rates com pared with placebo and are equivalent in head-to-head research. Combining glatiramer acetate with an interferon-beta pro vides no additional benefit to what both drug achieves alone. Natalizumab is a highly effective medication, decreasing relapse rates by approx imately two thirds compared with placebo over 2 years and slowing 2-year incapacity development by approximately 40%. It is run as an rare intravenous infusion (once per day for five consecutive days and then once more for three consecutive days 1 yr later). Because of serious security concerns (see Table 32), alemtuzumab administration requires intensive security monitoring and risk modification. Its increased danger of herpetic viral infections may be decreased with use of prophylactic antiviral brokers. Fingolimod is a as quickly as every day tablet that results in sequestra tion of activated lymphocytes in lymph nodes. Teriflunomide is a as quickly as every day pill that exerts an immuno suppressive impact by inhibiting a mitochondrial enzyme concerned in pyrimidine synthesis in rapidly dividing cells. Oral dimethyl fumarate exerts its immunomodulatory effects by modulating the nuclear factor-like 2 transcriptional pathway. Mitoxantrone is an anthracenedione chemotherapeutic agent that exerts an immunosuppressive effect by decreasing lymphocyte proliferation. For severe spasticity, botulinum toxin or implantable intrathecal baclofen pumps also can be used. Treatment of neuropathic pain frequently involves the use of lots of the identical drugs used to deal with painful diabetic neuropathy. Clinicians must be vigilant for signs of melancholy and have a low threshold for initiating antidepres sants and providing referrals to psychiatry and particular person or group remedy applications. Physical and occupational remedy is beneficial to ensure gait safely and enhance strolling ability and endurance. This treatment probably features hy ciccentua1i11g,rnd amplifying motion potentials. This symptolll manifests as uncontrolled f1ts of laughter or crying that occur without dis tincl or applicable triggers. A detailed sensory examination in suspected spinal cord injury is important, together with ascending pinprick testing all through the complete torso and neck, as a result of myelopathies usually end in a dis tinct sensory stage below which sensation may be altered or misplaced. This sometimes correlates anatomically with the level of harm and thus helps with localization and directed spinal imaging. Loss of perianal sensation specifically is a key finding that implies cauda equina syndrome. Gait is abnor mal in most patients with myelopathy and generally may be an isolated presenting check in gentle progressive myelopathy. Findings can range from a subtle spastic gait or sensory ataxia to complete paralysis. Many sufferers with myelopathy will report ache at the degree of the compressive illness. Some also describe squeezing or banding sensations across the chest or abdomen near the level of compression that sometimes result in unnecessary cardiac, pulmonary, or gastrointestinal evalua tions and delay in acceptable diagnosis. Patients also can expertise disruptions in bowel and bladder perform and loss of sphincter tone. Disorders of the Spinal Cord the important anatomy of the spinal twine and its susceptibility to injury due to its small diameter make recognizing and resolving spinal damage in a timely manner crucial. The presenting signs and symptoms of spinal twine injury often occur at or below the site of the lesion. When injury to the corticospinal tracts happens, spastic paresis or paralysis is feasible, manifesting as weak spot, hyperreflexia, muscle spasllls, and extensor plantar responses. Involvelllent of the distal spinal cord and lower roots (cauda equina syndrollle) 66 � Myelopathies often result in a distinct sensory degree beneath which sensation can be altered or misplaced, and this finding typically correlates anatomically with the level of harm and helps with localization and directed spinal imaging.
300 mg gemfibrozil order free shipping
Varying degrees of lung involvement and pathology could be seen in other types of connective tissue illness cholesterol medication for pregnancy gemfibrozil 300 mg buy without a prescription. Immune response to an inhaled low-molecular-weight antigen; may be acute cholesterol ratio of 4.2 gemfibrozil 300 mg discount without a prescription, subacute, or chronic. Systemic sclerosis Polymyositis/ dermatomyositis Other connective tissue illnesses Hypersensitivity pneumonitis Unknown Causes Idiopathic interstitial pneumonias Idiopathic pulmonary fibrosis Acute interstitial pneumonia C ryptogenic organizing pneumonia Sarcoidosis Chronic, insidious onset of cough and dyspnea, usually in a patient aged >50 y. Usual interstitial pneumonia pathology (honeycombing, bibasilar infiltrates with fibrosis). Dense bilateral acute lung harm much like acute respiratory distress syndrome; 50% mortality fee. Radiograph reveals focal areas of consolidation which will migrate from one location to one other. Variable medical presentation, ranging from asymptomatic to multiorgan involvement. Chest radiograph exhibits "radiographic negative" coronary heart failure, with peripheral alveolar infiltrates predominating. Other findings may embrace peripheral blood eosinophilia and eosinophilia on bronchoalveolar lavage. Median age of 39 years, and males predominate amongst smokers however not in nonsmokers. Diagnosed through bronchoalveolar lavage, which exhibits plentiful protein in the airspaces. For signs of shorter duration, lasting days to weeks quite than over months, infection and heart failure remain the most probably trigger. For each of these classes, the differential diagnoses overlap with the idio pathic interstitial pneumonias. Chest films could present increased intersti tial reticular or nodular infiltrates in several patterns of dis tribution, however they could be normal in as much as 20% of patients. There is little position for the usage of typical er imaging (5-mm slice thickness) for this popu lation given the limits of its decision. Outside of the lung parenchyma, additional findings could additionally be present in the mediastinum, pleura, and gentle tissues that help in making a prognosis. For instance, mediastinal and hilar lymphadenopathy is a common discovering in sarcoidosis, whereas considerably enlarged lymph nodes are a uncommon discovering in patients with idiopathic pulmonary fibrosis (! Cl Video assisteel thon1coscopic Jung biopsy is,1n nptinn for Surgical Lung Biopsy exposure and possible asbestosis. Smoking-Related Diffuse Parenchymal Lung Disease Desquamative interstitial pneumonia is as a result of of in depth, dif fuse macrophage filling of alveolar spaces with predominant cough and dyspnea symptoms and bilateral ground-glass opacities on chest imaging. Pulmonary Langerhans cell histio cytosis is characterized by thin-walled cysts with accompany ing nodules and is commonly related to pulmonary hypertension. For these with milder dis ease, pulmonary operate exams can be regular, restrictive, or obstructive. Although glucocorticoids are utilized in people with extra extreme illness, the profit of their use is uncertain. It is necessary to establish an underlying autoimmune disorder due to its impact on prognosis, drug therapy rec ommendations, and administration of comorbidities which will adversely have an effect on pulmonary outcomes. For instance, progressive pulmonary disease is now the pri mary explanation for mortality in systemic sclerosis. Cyclophosphamide may have some sho11-term profit in treating the lung illness, and managing the gastroesophageal dysmotility related to systemic sclerosis could assist keep away from aspiration and additional lung harm. Currently, these manifestations of rheumatoid atthritis are often handled with glucoc0t1icoids and disease-modifying agents; nonetheless, there are little knowledge to recommend clear efficacy for thjs strategy. Symptoms sometimes wane inside 2,1 � All sufferers with diffuse parenchymal lung disease should be clirucally assessed for an underlying autoimmune dis order because of its effect on prognosis, drug remedy rec ommendations, and management of comorbidities. Recurrence of symptoms with exposure to the respiratory antigen is the corridor mark or this clisorcler. Sub,1cute and continual types oflhe disease additionally occur ancl are believed to he associated with extra continual low-level exposures to inhaleci antigen. The primary 111anc1gement oft hese clisorclers is elimination or the ollencling agent. Cl Drug-Induced Parenchymal Lung Disease In sufferers who current with diffuse abnormalities on chest imaging. I lundreds or drugs have been described in affiliation with drug induced lung disease. Symptoms can deve lop acutely Radiation-Induced Parenchymal Lung Disease Symptoms or acute radiation pneumonitis typic ally happen 6 lo 12 weeks al"tcr publicity. Drug Amiodarone Select Drug-Induced Parenchymal Lung Diseases Clinical Points More widespread in: Older sufferers Increased dosage and better cumulative dose First year of remedy (but can happen late) Radiographic Findings and Treatment Multiple radiographic presentations potential together with ground-glass opacities, subpleural nodules, and reticular abnormalities Very lengthy half-life prevents clearance from the pulmonary parenchyma: Rare enchancment with discontinuation of the drug alone High danger of recurrence with tapering of glucocorticoids Methotrexate Occurs in less than 5% of sufferers handled Unpredictable time to presentation No clear correlation between dose and disease severity Diffuse reticular and ground-glass attenuation Patients typically do nicely after stopping treatment Glucocorticoids are often given and period is predicated on response Acute: Faint bilateral lower lobe septal strains; average pleural effusions could also be current. Treatment: Often will resolve with discontinuation however will recur with repeat exposure. Chronic: Reticular opacities with subpleural lines and thickened peri-bronchovascular areas. Some indi'idu,1ls 36 will have slowly progressive declines in their compelled very important c;ip,1city. Still others will clemonslrate stepwise declines in their pulmon,1ry perform exams with acute declines i<>llowed by subsequent stabilizalion. The most present fashions or discc1sc lclcus on I he interplay,1rnong,1lveolar cpitheli,11 cells. Some patients may initially current with solely pulmonary manifestations of their underlying autoimmune dysfunction. This cohort of patients ought to obtain continued surveillance for growth of connective tissue illness. A cautious review of methods is a key element of affected person follow-up; new-onset signs should immediate further diagnostic assessments. In general, the prognosis for patients with an underlying autoimmune disor der is better than these with! Nonspecific Interstitial Pneumonia � the latest evidence-based consensus statement recommends in opposition to mechanical ventilation for indi viduals with acute respiratory failure due to both development or an acute exacerbation of idiopathic pulmonary fibrosis. Patients m,1y additionally pre sent with a number of l,irge nodules or masses which may be preclorni n,111tly peripheral. Chest radiograph displaying cryptogenic organizing pneumonia with a quantity of patchy bilateral alveolar opacities which might be nonspecific and may be troublesome to distinguish from extra typical infectious pneumonia. Infiltrates could additionally be migra tory with resolution of established opacities as new areas appear on serial imaging. Imaging may be nonspecific, displaying interstitial infiltrates and alveolar opaci fication or displaying a quantity of rounded nodules that might be interpreted as malignancy. Individuals who recover from the initial illness may relapse or develop persistent lung disease. Chest radiograph showing stage I pulmonary sarcoidosis with hilar lymphadenopathy and regular lung parenchyma. Although this sue biopsy (most often via bronchoscopy with transbronchial and lymph node biopsy) is usually required to diagnose sar coidosis and exclude important different diagnoses. The determination to initiate glucocorticoid therapy for sarcoidosis should he primarily based on symptoms or physiologic impairmenl I h81 is 811Tih utable to sarcoid disease.
Gemfibrozil 300 mg trusted
Cl Cholangiocarcinoma cholesterol test new york city gemfibrozil 300 mg purchase with visa, or bile duct most cancers kind of cholesterol in shrimp discount gemfibrozil 300 mg online, is the second most typical primary malignancy of the liver after hepatocellu lar carcinoma. Established risk elements include major sclerosing chol angitis, choledochal cysts, the liver flukes Clonorchis and Opisthorchis, previous publicity to thorium dioxide distinction media, and hepatolithiasis. Presenting signs might include right upper quadrant ache, constitutional symptoms, or jaundice. Intrahepatic cholangiocarcinoma usually pre sents as a mass lesion within the liver, perihilar cholangiocar cinoma arises from the confluence of the best and left hepatic ducts (Klatskin tumor), and distal cholangiocarcinoma arises from the frequent bile duct, below the cystic duct insertion. Intrahepatic tumors are often asymptomatic until late-stage disease, which can current with right higher quadrant pain, constitutional signs, or an elevated serum alkaline phos phatase degree. Perihilar and distal tumors commonly current with jaundice and are related to a mass or dilated bile ducts above the lesion on imaging. Approximately 80% is as a result of of 4 causes: peptic ulcer illness, esophagogastric varices. Slow and/or chronic bleeding may be advised by history and iron defi ciency and is typical of erosive illness. A historical past of continual alcohol abuse is a clue Lo the chance of variceal bleeding. Causes and Prevalence of Upper Gastrointestinal Bleeding Cause Peptic ulcer Esophagogastric varices Erosive esophagitis Mallory-Weiss tear Erosion Tumor Esophageal ulcer Portal gastropathy Dieulafoy lesion Cameron lesion Other 33. Causes of Bleeding and Outcomes in Patients Hospitalized With Upper Gastrointestinal Bleeding. Hemobilia is usually due to a liver or biliary procedural complication but can also hardly ever be attributable to gallstone complications, tumors. Hemosuccus pancreaticus (blood emerging from the pan creas) is typically associated with pancrec1tic pseudocysts and pseudoaneurysm; it could additionally happen as a complication of endo scopic procedures, together with sphincterotomy. Outpatient management is often appropriate when the following standards are met: blood urea nitrogen level lower than 18. Patients ought to be resuscitated with crystalloids to attain physi ologic endpoints (pulse fee <100/min, systolic blood stress >100 mm Hg. Blood transfusion � Evaluation of acute gastrointestinal bleeding includes assessing severity, figuring out the need for interven tions, and differentiating between upper and decrease gasoline trointestinal bleeding sources. Octreotide and antibiotics must be administered before endoscopy for suspected variceal bleeding. Category la lb Ila lib lie Ill Endoscopic Evaluation and Treatment Courtesy of Louis M. Top panel: Clean-based gastric ulcer with no blood vessels, pigmented spots/protuber ances, or clots noted in the base (Forrest class Ill). Bottom panel: Gastric ulcer with non protuberant pigmented spot (arrow) in a duodenal ulcer bed (Forrest class lie). Local injection of the vasoconstrictor epinephrine could additionally be used adjunctively to assist instant hemostasis for optimizing visibility for subsequent and more durable endo scopic remedy; however, epinephrine injection alone is inad equate for durable hemostasis. Following endoscopic therapy, the strongest predictors of recurrent bleeding are hemodynamic instability. Bottom panel: Ulcer (solid arrow) with energetic arterial spurting (dotted arrow) (Forrest class la). This may be handled medically, or by clot elimination and endoscopic therapy in addition to normal medical therapy. Lower gastrointestinal bleeding sometimes happens in older indi viduals and presents as acute brilliant pink blood per rectum or red- or maroon-colored stool (hematochezia). Hemodynamic instability is much less widespread but, if present, raises the potential for a briskly bleeding upper gastrointestinal source. The alternative of whether to discontinue or withhold anti platelet brokers in sufferers with clear indications for remedy ought to stability the danger of rebleeding with the danger of throm bosis. Aspirin ought to be resumed within 3 to 5 days for sufferers with established cardiovascular disease. Aspirin reduces mor tality rates tenfold over 30 days whereas rising rebleeding charges only twofold. Patients taking aspirin and clopidogrel for coronary stents ought to proceed aspirin. In situa tions during which dual antiplatelet therapy is indicated (such as following placement of a drug-eluting stent). Patients with high thrombotic danger should receive reantico agulation but only after evaluating tlu�omboembolic threat in opposition to rebleeding threat. Causes Hematochezia is usually from a colonic source, however in approx imately 25% of patients the supply is in the upper gastrointes tinal tract, the small intestine, or an obscure location. Diverticula characterize herniation of mucosa/submucosa through the muscular layers of the colon. Diverticula are most commonly left sided, but colonic diverticular bleeding happens in either side of the colon. Causes and Prevalence of Lower Gastrointestinal Prevalence 24% 8% 6% 6% 3% 9% 3% 12% 30% 14% Jul; 15(7):333. Postpolypectorny bleeding is often related to use of electrocautery strategies for polypectomy and will have a delayed presentation. The prevalence of angiodysplasia will increase with age and may be overlooked during colonoscopy if bleeding has stopped. Direct evidence is missing to outline a transparent blood transfu sion technique for colonic bleeding. According to expe11 opinion, the blood transfusion threshold for patients with colonic bleeding is a hemoglobin value lower than 9 to 10 g/dL (90 to 100 g/L): the upper cutoff ought to be used when cardiovascular cornorbidities (including ischemic coronary heart illness, peripheral vascular surgery. Patients with suspected left-sided bleeding may endure anoscopy or sig moidoscopy as an preliminary analysis (particularly for colitis, rectal ulcer. Most sufferers require colonoscopy, nonetheless, even if a distal bleeding supply is suspected. Colonoscopy perfonned early is more more likely to identify a bleeding supply and allow for therapy. Submucosal epinephrine injection should be mixed with thermal or mechanical hemostatic methods. Data are lim ited for predicting outcomes based on endoscopic findings; a single center reported that diverticuar bleeding associated with major stigmata or hemorrhage (active bleeding. For failed endoscopic hemostasis or recurrent bleeding, the following therapeutic step is session with interventional radiology for arterial embolization of the bleeding source. Approximately 5% of" gastrointestinal bleeding has an obscure trigger occurring somewhere between the papilla and the ileocecal valve (also generally known as midgastrointestinal bleeding). If these tests are negative, the following step in a patient with continued bleeding is repeated endo scopic examinations (upper endoscopy. If the affected person is steady, observa tion with iron substitute is an inexpensive approach. At the top of the diverticulum is a visible vessel, which is the raised black spot at the top (arrow). Sources discovered by repeat con ventional upper endoscopy and colonoscopy embody Cameron ulcerations in a hiatal hernia. However, older patients are extra probably to have vascular lesions, such as angiodysplasia.
Gemfibrozil 300 mg generic line
Item fifty four Answer: B ll1e most appropriate management is laparoscopic cholecys Iectomy prior to cholesterol stones gemfibrozil 300 mg cheap on line hospital discharge cholesterol rating chart gemfibrozil 300 mg low cost. Bile acid dissolution remedy for gallstones has not gained widespread acceptance because most sufferers. In a research of pregnant women who had issues associated to gallstones during pregnancy, recurrent biliary signs. Causes of bleeding and out is out there in sufferers hospitalized with upper gastrointestinal bleeding. Conservative administration of cholelithiasis and its complications in pregnancy is associated with recurrent signs and more emergency department visits. Item fifty six Answer: D essentially the most acceptable management is to repeat colonos copy in three months. Invasive adenocarcinoma arising in a pedunculated polyp may be considered adequately handled by endoscopic en bloc polypectomy alone if the lesion is confined to the sub mucosa and possesses no antagonistic histologic options corresponding to poor differentiation, lymphatic or vascular invasion, or involved margins. National suggestions for postpolyp ectomy surveillance intervals are as brief as 3 to 6 months in sufferers with large (>2 cm) adenomas or adenomas with invasive most cancers and favorable prognostic options. These shorter surveillance intervals help to be certain that no residual polyp tissue stays. If any antagonistic histologic features are noted, the chance of lymph node involvement is elevated substantially and surgical resection of the involved colon is required. Item fifty seven Answer: D Bibliography probably the most applicable test to carry out subsequent is angiography. Latex balloons are mounted on an overtube that may deliver the enteroscope into the small bowel by successive in nation and denation. Balloon enteroscopy can deliver the enteroscope orally or rectally (retrograde) and can be utilized for analysis and therapy. Complications of balloon enteros copy are perforation and bleeding by way of avulsion of� the bowel. Endoscopic retrograde cholangiopancreatography with sphincterotomy can be a consideration if this affected person had gallbladder stones and/or a typical bile duct stone. Emergent cholecystostomy is superior to open cholecystectomy in extraordinarily ill patients with acalculous cholecystitis: a big multicenter consequence research. This is known as acalculous cholecysti this and is believed to replicate either bacterial seeding of the gallbladder wall or gallbladder wall ischemia. Fever accompanying stomach ache in a critically ill affected person ought to prompt an evaluation for cholecystitis. Diagnosis is often made with ultrasound findings of acute chole cystitis or a radionuclide biliary scan that fails to visualize the gallbladder. Definitive remedy with cholecystectomy is most well-liked however may be contraindicated in severely sick sufferers. Therapeu tic decompression can be achieved with image-guided percutaneous cholecystostomy tube placement. Blood transfusion must be performed in sufferers with (1) hemodynamic instability and ongoing bleeding or sus ceptibility to problems from oxygen deprivation (for instance. Item 60 Answer: D � Low-risk gastric ulcers are clean-based or have a non protuberant pigmented spot; they need to be handled with oral proton pump inhibitor therapy, initiation of refeeding within 24 hours, and early hospital discharge. A prognosis of hepatocellular carcinoma could be made in a patient with cirrhosis within the presence of lesions bigger than 1 cm that improve in the arterial phase and have washout of distinction in the venous section. Patients who meet the Milan criteria (up to three hepatocellular carcinoma tumors 3 cm or one tumor 5 cm) have excellent 5-year survival charges after liver transplantation. The vast majority of hepatocellular carcinomas in the con text of cirrhosis can be recognized with radiologic criteria alone. There is also a small risk (1%-3 %) of seeding the needle monitor with tumor cells with percutaneous biopsy of hepato cellular carcinoma. Sorafenib, a compound that targets growth signaling and angiogenesis, ought to be reserved for patients with Child Turcotte-Pugh class A or B cirrhosis, good efficiency standing, and vascular, lymphatic, or extrahepatic spread of the tumor. This affected person has no evidence of angiolymphatic or extrahepatic involvement, and the tumor sizes are inside Milan criteria; due to this fact, he ought to be evaluated for liver transplantation somewhat than began on sorafenib. Preventive Services Task Force really helpful screening for hepatitis C once in all persons born between 1945 and 1965, as well as focused screening of individuals with danger components similar to illicit drug use, receipt of blood prod ucts, hemodialysis, and a number of intercourse partners. The patient has already been diagnosed with the two mutations; subsequently, both his mother and father must be constructive for the mutation. Therefore, prophylactic antibiotics must be offered for patients with cirrhosis and variceal hemorrhage, whatever the pres ence or absence of ascites. Intravenous ceftriaxone could additionally be more eflective for patients with Child Turcotte-Pugh class Band C cirrhosis. A nonselective -blocker is recommended as secondary prophylaxis after restoration from a variceal bleed, however it might not be warranted within the acute setting in this patient with hypotension. An upper endoscopy must be performed on this affected person with presumed variceal hemorrhage within 12 hours, however only after she has been treated with normal phar macotherapy (octreotide and antibiotics) and appropriately resuscitated to enable safe endoscopy. A blood pressure of 72/54 mm Hg is too low to be in a position to proceed immediately with a secure endoscopy. This patient has decompensated cir rhosis as evidenced by earlier ascites and jaundice. A frequent misperception is that anti biotic prophylaxis want only be provided for sufferers with variceal hemorrhage and ascites (at risk for spontaneous bacterial peritonitis). A Cochrane systematic evaluation con firmed that antibiotic prophylaxis throughout variceal bleeding not only helps prevent spontaneous bacterial peritonitis but additionally helps reduces the danger of bacteremia. Meta-analysis: antibiotic prophylaxis for cirrhotic sufferers with upper gastrointestinal bleeding - an updated Cochrane evaluate. This affected person has the combination of free stools, unintentional weight loss, elevated liver chemistry check results, and iron deficiency ane mia without an obvious supply of blood loss. Minor elevations of serum aminotransferase levels are found in as much as 50% of sufferers with celiac illness and will be the solely presenting function in approximately 9% of sufferers. Patients with celiac illness can also have coexisting liver illness corresponding to autoimmune hepatitis, primary sclerosing cholangitis, or main biliary cirrhosis. Improvements in liver chemistry 141 Educational Objective: Diagnose celiac illness in a affected person with irregular liver chemistry studies. Item sixty five Answer: B Answers and Critiques research which may be associated to celiac disease occur when such patients are treated with a gluten-free cliet. Additional findings of chol angitis embody jaundice and ache in the proper upper quad rant (Charcot triad). Sphincter of Oddi dysfunction would produce the identical symptoms as are discovered on this affected person: however. Educational Objective: Diagnose a common bile duct � Celiac illness is identified in 9% of patients with oth erwise unexplained elevated serum aminotransferase ranges. Replacing the meto clopramide with a scheduled antiemetic is the safest and most cost-effective subsequent step in administration. The initial therapy of diabetic gastroparesis should embody a dietary administration plan consisting of frequent small-volume meals which would possibly be low in fat and soluble fiber.
Real Experiences: Customer Reviews on Gemfibrozil
Felipe, 49 years: Roflumilast is contraindi cated in sufferers with liver impairment and has vital drug interactions. He reviews feeling significantly better, with decreased shortness of breath and cough; he has been afebrile because the second hospital day.
Taklar, 43 years: In addition to analysis for liver transplantation, which of the next is probably the most acceptable remedy Resistance testing should all the time be done before an initial drug regimen is chosen and when treatment failure occurs, as indicated by failure to suppress viral load or an increase in viral load that was beforehand suppressed.
Osko, 26 years: Use of a break up dura for revascularization of ischemic hemispheres in moyamaya illness. The epidemiology, prognosis, and administration of aristolochic acid nephropathy: a story evaluate.
Stan, 22 years: There are two major forms of abnormalities that affect the pleura: elevated fluid (pleural effusion) and air (pneumotho rax) within the pleural house. Connective tissue changes associated with prior head and neck radiation remedy might make airway management difficult.
Jack, 65 years: In particular, hypertension is the strongest threat factor for hemor rhagic and ischemic stroke. It typically occurs concurrently with an underlying congenital disease in children, whereas in adults an acquired underlying disease is frequent.
9 of 10 - Review by H. Rasul
Votes: 173 votes
Total customer reviews: 173
