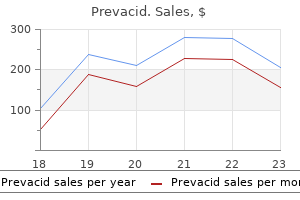
Prevacid dosages: 30 mg, 15 mg
Prevacid packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Generic prevacid 15 mg without prescription
Increased serum levels of elastase have additionally been observed in sufferers with aneurysms gastritis symptoms list buy prevacid 15 mg overnight delivery. Cathepsin D is an endopeptidase that may also digest extracellular matrix proteins gastritis recovery diet prevacid 30 mg order fast delivery. Data recommend that elevated proteolysis can also contribute to rupture of intracranial aneurysms. In distinction, many apoptotic cells are present in intracranial aneurysm walls, particularly in ruptured aneurysms. These outcomes recommend that apoptosis plays an essential position within the improvement and rupture of intracranial aneurysms. It had been proposed that apoptosis is induced by cytokines released by inflammatory cells that infiltrate aneurysm tissues. These information suggest that hemodynamic stress results in arterial wall degeneration and ultimately to aneurysm formation. Although the intracranial aneurysms in these fashions appear to form at areas of excessive hemodynamic stress, corresponding to arterial bifurcations, research on intra-aneurysmal hemodynamic circulate in human intracranial aneurysms have shown that aneurysm progress is associated with low shear stress. In measuring intra-aneurysmal flow in three aneurysm models, Yamaguchi and coauthors92 showed that larger facet ratios (dome/neck measurement, known to be correlated with rupture) are associated with low wall shear stress. Jou and colleagues93 retrospectively analyzed wall shear distribution in 8 ruptured aneurysms and 18 unruptured inner carotid aneurysms and located that in ruptured aneurysms, a larger proportion of the aneurysm was exposed to low wall shear stress. Marker Control artery #1 #6 Aneurysm #9 #8 Control artery #1 #6 Aneurysm #9 #8 Atherosclerosis and Intracranial Aneurysms zero. Hemodynamic Stress and Intracranial Aneurysms Intracranial aneurysms have been induced by hypertension and carotid ligation in animal fashions. Such adjustments include fragmentation of the interior elastic lamina, thinning of the the presence of atherosclerotic plaque in some intracranial aneurysms and the similar histologic and biochemical options of aneurysmal and atherosclerotic lesions counsel that atherosclerosis may be a mechanism in the pathogenesis of intracranial aneurysms. Furthermore, intracranial aneurysm and atherosclerosis have threat factors in common, similar to smoking and hypertension. Immune and adaptive immune responses are activated in atherosclerotic lesions, together with infiltration of macrophages, T cells,94-96 B cells,97 mast cells,98,ninety nine and natural killer cells100; binding of antibodies101; and activation of complement. Macrophages additionally induce the production of progress elements and more cytokines by activating T cells and B cells. Oxidative stress and free radicals in atherosclerotic walls can also activate the immune response. Several research assist the hypothesis that aneurysm formation and atherosclerosis may be associated. In a histologic examination of atherosclerotic saccular aneurysms, Kosierkiewicz and coworkers46 discovered that aneurysm measurement is said to the development of atherosclerotic plaque. In small aneurysms, atherosclerotic lesions have been characterised by intimal thickening with solely minimal inflammatory cell infiltration. In giant aneurysms, atherosclerotic lesions were more superior and exhibited extra in depth macrophage, lymphocyte, and pure killer cell infiltration. In a research involving 50 sufferers with intracranial aneurysms and no vital atheromatous disease, Bolger and associates106 found that elevated serum levels of lipoprotein (a) (Lp[a]), an impartial risk issue for atherosclerosis, had been additionally detected in sufferers with aneurysms, whose common serum Lp(a) ranges were twofold larger than those in wholesome normal controls. These knowledge suggest that Lp(a) can be associated with the presence of intracranial aneurysms. In an investigation of the wall shear stress distribution between areas with and with out atherosclerotic modifications in a single, massive center cerebral artery aneurysm, Tateshima and colleagues107 confirmed that low wall shear stress was correlated with the presence of atherosclerotic areas. Increased expression of phosphorylated c-Jun amino-terminal kinase and phosphorylated c-Jun in human cerebral aneurysms: role of the c-Jun amino-terminal kinase/c-Jun pathway in apoptosis of vascular partitions. In an autopsy research of six intracranial aneurysms, Hassler38 detected slight atherosclerotic adjustments near the neighborhood of the aneurysms. However, no obvious relationship between the presence of atherosclerosis and aneurysms was found. Although elevated Lp(a) ranges had been associated with intracranial aneurysm formation (described earlier), examination of Lp(a) expression in intracranial aneurysm samples and management arteries with and with out atherosclerosis confirmed that Lp(a) expression in aneurysms may happen independently of atherosclerosis. Identifying causative genetic mutations is important for obtaining a deeper understanding of the pathogenesis of aneurysm formation and has been a spotlight of analysis because the early 2000s. From work in our laboratory, a susceptibility area in chromosome 13q was famous via the use of a genome-wide linkage strategy in a single, large white family with autosomal dominant intracranial aneurysms. Squares represent male members of the family; circles represent female relations; black symbols symbolize affected persons; white symbols represent unaffected individuals; gray symbols represent unknown phenotype; plus indicators indicate R450X mutation carriers; and minus signs point out noncarriers. Triangles characterize predicted N-glycosylation sites; circles represent predicted phosphorylation websites. This aneurysm is termed saccular as a end result of the neck (black arrow) arises from an arterial department level, the inner carotid artery (at the base of the aneurysm neck), and the opthalmic artery (red arrow). Red arrow signifies superior cerebellar artery; black arrow indicates the neck of the aneurysm arising from the trunk of the artery, not at its origin from the basilar artery (white arrow). Because this aneurysm arose from the trunk and not a branch point, it was categorized as fusiform. Severe hydrocephalus results in intracranial hypertension and poor cerebral perfusion. In wild-type animals, no ventricular dilatation was observed, and the vessels of the circle of Willis and emerging small vessels were well delineated. D, the brain of a Thsd1Venus/+ mouse that died all of a sudden at age 9 weeks and that of a wild-type mouse sacrificed at 9 weeks. Both brains have been from nonperfused animals and imaged beneath the identical dissecting microscope. Unlike the wild-type brain, the Thsd1Venus/+ brain showed massive and diffuse cerebral hemorrhage. E, Hematoxylin and eosin staining of mind slices from wild-type, Thsd1Venus/+, and Thsd1Venus/Venus mice. These pictures present enlargement of lateral ventricles and extravasation of blood into the subarachnoid space (asterisk) in a subset of animals with the mutation. Focal adhesions are giant, specialized, dynamic constructions in which actin filament bundles are anchored to transmembrane integrin receptors by way of an meeting of proteins. Integrins bind to extracellular proteins, and inside the cell, the intracellular domain of integrins binds to the actin filament bundles through adapter proteins similar to talin, -actin, paxillin, and vinculin. In addition to anchoring the cell, focal adhesions function as signal carriers that may affect mobile habits. Further evidence that cell adhesion performs a major position comes from an intriguing Finnish research. Further investigation confirmed that two siblings had died of ruptured intracranial aneurysms. Although no additional genetic evaluation was performed on this household, this specific translocation causes breakage of intron 1 of a splicing isoform of neurotrimin. The neurotrimin gene is expressed within the central nervous system and encodes a cell adhesion molecule.
Bitter Almond Oil (Bitter Almond). Prevacid.
- How does Bitter Almond work?
- Dosing considerations for Bitter Almond.
- Are there any interactions with medications?
- Are there safety concerns?
- What is Bitter Almond?
- Spasms, pain, cough, itch, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96335
Generic prevacid 30 mg free shipping
Mechanical testing of unfixed human cerebral arteries harvested inside 12 hours of death exhibits irreversible plastic deformation with inflation pressures in the vary of zero chronic gastritis stress order 30 mg prevacid free shipping. However gastritis diet ���� discount prevacid 30 mg without prescription, when balloons are constrained by constricted arteries, the inflation pressure can rise dramatically with every further increment of inflation volume. As with all kinds of hemorrhagic complications, anticoagulation should be reversed as rapidly as possible with protamine. Intracranial hypertension ought to be managed medically and with ventricular drainage as necessary. Control angiography ought to be performed via the information catheter to assess hemostasis while the balloon is inflated. If bleeding persists across the balloon, the surgeon ought to think about repositioning the balloon or putting a second balloon. Depending on the affected vessel, sacrifice by coil embolization may be necessary but may be incompatible with an appropriate consequence. If essential, a second embolization-capable microcatheter should be used whereas the balloon remains in place. In some instances, sustained balloon occlusion for 30 to 60 minutes produces durable hemostasis that continues after the balloon is deflated. In different circumstances, the rupture is transformed to a pseudoaneurysm, which may be amenable to coil embolization with or and not utilizing a stent for vessel reconstruction. In our expertise, such pseudoaneurysms are troublesome to control by coil embolization alone. Embolization with a combination of coils and a liquid embolic agent, performed in a balloon remodeling method, is extra more doubtless to be successful. Longer balloon lengths that extend across the whole remedy segment are advantageous in that they limit the variety of inflations essential to complete therapy. This avoids repetitive harm to transition segments bridging sequentially dilated segments and prevents lack of balloon radiopacity (visbility) when single-lumen balloon catheters are used. When successive dilations are carried out, they should be accomplished in the distal-to-proximal direction, which avoids instrumentation of freshly dilated segments. Treatment paradigms will continue to evolve as new medicines become out there, diagnostic modalities are found, and the pathophysiologic characteristics of vasospasm are better understood. Because of those promising future developments, vascular neurosurgeons and interventionalists should remain attuned to such modifications and tailor treatment regimens accordingly. American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Comparison of balloon angioplasty and papaverine infusion for the treatment of vasospasm following aneurysmal subarachnoid hemorrhage. Intracranial strain adjustments induced during papaverine infusion for remedy of vasospasm. Intracranial pressure monitoring throughout intraarterial papaverine infusion for cerebral vasospasm. The efficacy and safety of angioplasty for cerebral vasospasm after subarachnoid hemorrhage. Effect of intraarterial verapamil on the diameter of vasospastic intracranial arteries in patients with cerebral vasospasm. High-dose intraarterial verapamil in the therapy of cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Intraarterially administered verapamil as adjunct therapy for cerebral vasospasm: safety and 2-year expertise. The prophylactic use of transluminal balloon angioplasty in sufferers with Fisher grade 3 subarachnoid hemorrhage: a pilot examine. Both therapy modalities are viable choices, and as each patient is different, so is each aneurysm. The determination to treat and which method of remedy to use is complicated and involves consideration of the natural historical past of cerebral aneurysms (see Chapter 377), traits of the affected person and the aneurysm, and the dangers involved in any therapy (see additionally Chapter 379). Understanding the dangers entails familiarity with the standing of current techniques of treatment. As already noted, many of these issues are extensively reviewed in other chapters (see Chapters 379 and 384-398). Another necessary factor within the success of remedy is a skull base method to the aneurysm, which, by elimination of enough bone, makes less retraction needed. Proximal and Distal Control Securing control of blood circulate each proximal and distal to the aneurysm being treated serves to forestall devastating hemorrhage within the event of intraoperative rupture and in addition softens the aneurysm, thereby aiding in perianeurysmal dissection and eventual clip placement. In many aneurysms of the anterior circulation, proximal and distal management could additionally be completed with relative simplicity by dissection of the father or mother artery proximal and distal to the aneurysm in question and placement of a temporary clip at both locations. Temporary clips have a less aggressive closing drive than do permanent clips, which prevents harm to or dissection of the artery being clipped. In some circumstances, nonetheless, proximal control of the father or mother vessel may be impractical because bone or other anatomy obscures the proximal portion of the parent vessel. In these cases, various techniques are often employed to lower blood circulate to the aneurysm. Thus dissection of, and maneuverability within, the subarachnoid area are basic in cerebrovascular surgery. Particularly within the setting of subarachnoid hemorrhage, this dissection may be made difficult by the presence of hemorrhagic byproducts, inflammatory reactions, fibrinous adhesions, and, sometimes, edema that renders the brain immune to manipulation. Hydrocephalus is usually related to a subarachnoid hemorrhage, and a ventriculostomy on the alternative side of the craniotomy will successfully deal with this affiliation. In other instances, as in the interhemispheric approach to aneurysms of the pericallosal artery (to be described), gravity might assist with brain mobilization, in such a method that additional mechanical retraction is often not required. The surgeon may successfully scale back brain swelling by administering intravenous hypertonic solutions or pharmacologic metabolic suppressive agents. The majority of intracranial aneurysms, nevertheless, may be approached and handled with the utilization of a minimal number of cranial approaches, each of which could be modified in a wide range of methods to suit the particular structure of the aneurysm being handled. A, Pterional craniotomy for strategy to aneurysms of the center cerebral artery; skin incision is represented by dashed purple line, bur holes by yellow circles, and the craniotomy by blue dashed line. B, Pterional craniotomy depicting intracranial view of an aneurysm within the center cerebral artery after craniotomy. Positioning the patient is positioned supine with a shoulder roll beneath the ipsilateral shoulder. The head is positioned in three-point pin fixation, rotated 10 to forty five degrees to the contralateral side, and translated anteriorly. The vertex is then rotated 10 to 20 levels towards the floor, which places the malar eminence at the highest point of the operative area and permits gravity to pull the frontal and temporal lobes away from the sylvian fissure, in order that less frontal and temporal lobe retraction is important. Some surgeons choose to bluntly dissect the airplane between the galea and temporalis fascia/pericranium earlier than incising the galea on this area, in efforts to stop inadvertent entry into the temporalis muscle, which might make reapproximating the muscle slightly harder throughout closure. The strategies by which the temporalis muscle could additionally be incised, mobilized, and retracted are quite a few; every has its personal virtues and limitations. The temporalis fascia could also be incised inferior to the superior temporal line and at the posterior side of the skin incision (leaving a cuff of muscle fascia in each areas to help with muscle fascia reapproximation throughout closure), and both scalp and temporalis muscle could also be elevated as one unit, both being mirrored anteriorly. This methodology ensures the protection of the frontalis branch of the facial nerve, nevertheless it has been criticized as a end result of the bulkiness of the temporalis muscle itself limits visualization along the sphenoid ridge.
Prevacid 30 mg generic overnight delivery
Carotid entry is gained directly via a supraclavicular incision and insertion of the working sheath gastritis from alcohol 15 mg prevacid sale, which thereby avoids catheter manipulation (and potential launch of embolic debris) in each the aortic arch and the proximal frequent carotid artery gastritis h pylori prevacid 15 mg cheap. The system was successfully utilized in 99% of 141 patients enrolled within the study. Its major use thus far has been to define the extent of plaque formation and consider plaque structure as a method to establish so-called susceptible plaque. We have discovered it helpful during poststenting deployment and poststenting angioplasty to consider for correct stent growth and intrastent or intraluminal thrombus (Video 367-2). When thrombus is identified, we sometimes use mechanical aspiration to remove friable intraluminal fragments, thereby eliminating the prospect of distal embolization. Intravascular ultrasonography revealed important stenosis, which was subsequently treated by angioplasty. Intravenous hydration ought to be maintained for as much as 24 hours after the procedure. Postprocedure hypotension must be aggressively managed with vasoconstrictors such as phenylephrine (Neo-Synephrine) or intravenous infusion of dopamine. Carotid artery disease is incessantly related to coronary artery disease, and sustained hypotension is a harbinger of myocardial ischemia. If a closure gadget has not been used, the arterial sheath must be removed when the activated coagulation time exceeds one hundred fifty seconds. In this method, direct entry to the carotid artery is obtained via a small incision made between the clavicular heads of the sternocleidomastoid muscle (A). The carotid sheath is related to a move regulator and filter, which is continuous with a sheath inserted in the femoral vein. In this way, blood flow is briefly diverted away from the mind during therapy. Debris created during the process is directed away from the brain (B) and trapped within the filter, and debris-free blood is returned into the femoral vein, which thereby decreases blood loss. All sufferers routinely undergo cardiac enzyme and electrocardiographic review before discharge. Duplex sonographic evaluation should be obtained before discharge, at 6 weeks, at 3 months, at 6 months, at 1 12 months, after which yearly thereafter. The twin antiplatelet routine of aspirin and clopidogrel (or ticlopidine) is maintained for 12 weeks after the procedure, after which sufferers remain on aspirin therapy. In a retrospective research of sufferers undergoing stenting for carotid stenosis, both de novo (119 arteries) and postendarterectomy (76 arteries), restenosis of 80% or extra was detected with Doppler imaging in 5. Thereafter, the chance falls considerably, remaining low throughout these studies. During the 4-year research period, the composite major end point-any periprocedural stroke, myocardial infarction, or death or postprocedural ipsilateral stroke-occurred in 7. In addition, a sudden decline in blood pressure or the onset of severe bradycardia, as may occur throughout stent placement or angioplasty, may present a serious risk for myocardial infarction in sufferers with severe illness of the left major coronary artery or extreme triple-vessel illness. Specifically, the presence of large-territory infarction poses a significant danger for hemorrhage. High-risk anatomy contains iliofemoral illness, calcified or tortuous aortic arches, and tortuosity or kinking of the frequent or inner carotid artery (Table 367-5). Therefore, the surgeon should evaluate every case on an individual foundation, weighing the dangers and advantages for each patient. When treatment is deemed necessary, artistic endovascular solutions may be discovered even for patients at high danger for problems. For patients with intraluminal thrombus and symptomatic carotid artery disease, the standard remedy has been heparin and warfarin therapy with reevaluation in 6 weeks to three months. Flow-reversal techniques also might prove helpful on this setting and in the context of kinks that preclude the landing of a distal embolic safety device. DirectCarotidAccess Direct carotid access has its personal set of potential problems. The inside jugular vein is positioned adjacent to the carotid artery; inadvertent damage to the vein can usually be managed with manual stress. For percutaneous carotid access, the use of ultrasonography may help distinguish the artery from the adjacent vein. Complications associated with access through carotid cutdown are similar to these seen in other anterior cervical approaches in neurosurgery. However, because the cutdown is directed toward the widespread carotid artery, quite than the bifurcation, the risk of injury to the cranial nerves is decreased. Manipulation of the cervical strap muscular tissues may trigger swelling and postprocedure pain. However, the event of a postprocedure hematoma should be recognized and managed aggressively as a end result of it has the capacity to cause airway compromise. Because approximately 33% of patients have both significant carotid artery disease and severe symptomatic peripheral vascular illness,108,109 the operator also needs to be acquainted with radial and brachial approaches. The true incidence of access web site issues is unknown because these are usually not recorded in main carotid stent trials. Micropuncture kits, single wall puncture, and femoral angiography to consider access web site anatomy and disease mitigate many of those complications, including dissection, occlusion associated to the closure device, and groin or retroperitoneal hematomas. GuideCatheterPlacement the exterior carotid artery and its branches are sometimes used to assist a guidewire during the exchange of a diagnostic catheter for a guide sheath or catheter. This maneuver is assumed to be safer than exchanging devices throughout the common carotid artery as a end result of it prevents premature crossing of the lesion and showering of emboli. The 4 wire perforations had been secondary to advancement of the stiff change wire through the facial artery (two cases), the lingual branch (one case), and the artery to the sternocleidomastoid artery (one case). These resulted in hematomas that responded to manual stress in a single case; necessitated embolization with n-butyl cyanoacrylate (glue) or coils in two cases; and necessitated emergency tracheostomy for airway control secondary to huge tongue swelling in a single case. First, massive branches of the exterior carotid artery, ideally the interior maxillary artery or occipital artery, must be used for change maneuvers. Second, rupture of a department of the carotid artery can lead to life-threatening airway emergencies. A doctor who can intubate the affected person or carry out an emergency tracheostomy to establish an airway must be readily accessible. Third, carotid interventionists need to be comfy with microcatheters and embolic agents similar to n-butyl cyanoacrylate, coils, silk, Gelfoam (Pfizer, New York), and even autologous clot as a way to stop bleeding from vessel perforations. Although a uncommon occasion, perforation of a branch of the exterior carotid artery can rapidly result in airway compromise if not recognized and treated promptly. An equally rare event is external carotid artery embolism to carotid ophthalmic collateral vessels, which may result in retinal embolism and blindness. Anatomically, this could occur via a number of avenues: (1) center meningeal and superficial temporal collateral vessels to the ophthalmic artery, (2) after internal carotid artery reconstitution, and (3) retrograde embolization via the external carotid artery to ophthalmic and retinal AorticorBrachiocephalicAccess In the method of obtaining access to the frequent carotid artery with a information catheter, damage to any of the most important aortic branches and brachiocephalic vessels can occur and lead to dissection, thrombotic occlusion, embolic infarction, or a combination of these.
30 mg prevacid buy with amex
Generally gastritis diet apples discount 30 mg prevacid amex, sufferers who stroll independently before therapy achieve this after treatment gastritis and ulcers prevacid 30 mg cheap without prescription. Dural arteriovenous malformations of the backbone: scientific features and surgical leads to 55 instances. B, Superselective angiogram through the microcatheter near the purpose of fistualization further defining the anatomy. On the left is a picture immediately before the injection of Onyx (the white arrows point out the place of the microcatheter tip). The proper image is a fluoroscopic picture by which the radiopaque Onyx is seen to penetrate the fistula into essentially the most proximal portion of the draining vein (black arrow). D, Final angiogram after the microcatheter was eliminated demonstrating complete obliteration of the fistula. Gentle retraction with a microsucker (with the tip of a small neurosurgical cotton patty and suction on low setting), dissection with the information of the bipolar forceps within the gliotic plane between the malformation and the spinal cord, and elevation of the malformation while working from one pole upward or downward to expose, coagulate, and interrupt the vessels coming into and leaving the malformation ventrally result in dissection of the nidus of the malformation from the encircling spinal wire. Generally, at least one of many major draining veins is preserved patent until dissection around the periphery of the malformation has been completed and all feeding vessels have been occluded. All patients have been treated by laminectomy, and 14 of 15 patients underwent full resection that was documented on immediate postoperative arteriography. Asymptomatic recurrences have been noted in 3 (23%) patients on later imaging studies, and the long-term obliteration fee at a mean of eight. Symptom onset ranged from 2 days to eleven years before surgery, and sufferers presented with subarachnoid hemorrhage (4 patients), intramedullary hematoma (2), paresthesias or ache (4), and myelopathy (10). Twenty p.c of patients suffered neurological deterioration after surgical procedure, which had resolved on follow-up. Of the 14 patients who received a postoperative arteriogram, complete obliteration was demonstrated in 11. Velat and associates reported good radiologic and medical outcomes in 20 patients, 17 of whom have been treated with the pial resection technique. Additionally, within the setting of acute and rapidly worsening neurological operate, typically a results of hemorrhage, surgical intervention appears to stabilize neurological perform in lots of patients. It have to be acknowledged that long-term follow-up that features scientific and arteriographic assessment for patients treated by microsurgical resection is lacking, and the incidence of arteriographic recurrence and medical relapse in incompletely resected lesions is undefined. For purposes of defining remedy protocols, Merland and colleagues categorized perimedullary fistulas based mostly on the caliber, length, and number of feeding and draining vessels (Table 414-5). Most trendy reports of microsurgical resection additionally embrace the usage of adjuvant embolization. Generally, patients who walked independently earlier than treatment do so after treatment. These fistulas reveal gradual move that ascends through the coronal venous plexus and leads to solely minimal venous dilation and tortuosity. There are multiple discrete shunts draining right into a dilated and tortuous venous system. The feeding vessels are extraordinarily dilated and converge right into a single shunt that drains into a giant venous ectasia. However, microsurgical obliteration is generally considered to be safer, more dependable, and sturdy, notably for posterior or posterolateral fistulas. In sufferers presenting with extreme neurological deterioration or progressive signs, surgical resection should be thought-about. However, in patients with only delicate signs or asymptomatic lesions, indications for surgical resection are much less clear as a result of the data on the natural historical past that exists means that by the way discovered cavernomas have a relatively safe pure history with out remedy. Of the surgical patients, 12 improved postoperatively, 2 remained steady, and three deteriorated. Importantly, the 3 patients managed conservatively demonstrated a steady neurological examination over a follow-up of three to 9 years. Bian and coworkers reported postoperative enchancment of signs in 16 sufferers with symptomatic spinal wire cavernous angiomas. Patients presenting with rapid deterioration from Foix-Alajouanine syndrome are at risk for everlasting disabling neurological harm from venous hypertension and venous thrombosis. Transarterial embolization allows for a rapid occlusion of the feeding pedicle and quick discount of venous hypertension until definitive microsurgical intervention may be performed, if needed. SurgicalTechnique Most cavernous angiomas are amenable to resection by the posterior approach. Lateral and anterolaterally positioned lesions can be accessed with costotransversectomy, sectioning of the dentate ligaments, and mildly rolling the wire to the contralateral aspect. Cavernous angiomas of the posterior half of the wire are associated with a lower incidence of iatrogenic damage throughout surgical procedure and a greater scientific prognosis than ventrally located lesions. Following dural opening, cavernous angiomas that extend to the cord floor are identified by hemosiderin staining and blue discoloration of the pia. The pia is opened, ideally where the mass presents to the floor, and dissection proceeds in the gliotic aircraft. The bipolar forceps are used to coagulate the floor of the lesion and collapse it inward. At the margins, the cavernous angioma may be adherent to the encircling tissue, and the lesion may have to be eliminated in multiple items. Complete resection is important as a end result of residual items of cavernous angioma usually result in symptomatic rehemorrhage. A third administration was given to evaluate for residual shunting within the resection mattress. Outcomes Postsurgical outcomes are largely dependent on preoperative neurological function (Table 414-6). Additional data recommend that sufferers with a chronic historical past (>3 years) of symptoms earlier than resection fare worse than patients with a shorter duration of symptoms126; 15% to 25% of surgical patients expertise a worsening neurological deficit instantly following surgical procedure. However, generally, the postoperative deficits resolve and sufferers exhibit improvement or stabilization. Maslehaty and colleagues retrospectively reviewed 14 patients with symptomatic spinal cavernous angiomas treated with microsurgical resection125; 7 sufferers demonstrated speedy improvement postoperatively, whereas the remaining 7 sufferers slowly improved and reported a good consequence. Steiger and associates reported 20 clinically symptomatic patients treated with either conservative management (3 patients) or microsurgical resection (17 patients). Intraoperative Arteriography Intraoperative arteriography provides evaluation of blood move, highlights relationships between feeding arteries and draining veins, and defines the complicated angioarchitecture of spinal vascular malformations. Disadvantages embrace that it may be time-consuming and technically tough with sufferers within the prone place. However, lengthy metal sheaths that can be exposed alongside the buttocks improve the benefit with which the process can be performed. She had an abrupt onset of severe headache, stiff neck, and weak spot and numbness of the left higher and decrease extremities 11 days earlier than admission. Note that in D the coiled, dilated arterialized veins conceal the site of the fistula and obscure visualization of the aneurysm. To cut back blood move through the fistula, a coil was positioned in the distal portion of the principal feeding artery, a posterior spinal artery, just proximal to the small aneurysm (G, arrow) the day earlier than the fistula was interrupted surgically and the large varix was excised. At surgical procedure, opening of the dura and arachnoid (J) uncovered the extramedullary varix (white arrow), the blue-gray shade of an intramedullary varix simply beneath the pia (black arrow), and the tortuous arterialized veins overlying the spinal twine superiorly. The tortuous arterialized veins covering the extramedullary portion of the patent a half of the aneurysm (J, white arrow) have been dissected free and displaced superiorly.
Cheap 15 mg prevacid with visa
Some patients might develop sclerotomal pain that radiates into the Disc herniation the nucleus pulposus in a degenerated disc might prolapse and push out from the weakened annulus gastritis diet what to eat generic prevacid 15 mg amex, usually posterolaterally gastritis vomiting blood prevacid 30 mg generic mastercard. Rarely, a big midline disc herniation, often L4�5, compresses the cauda equina. This is a surgical emergency because neurological outcomes are affected by the time to decompression. Whenever attainable, the cauda equina syndrome ought to be acknowledged before incontinence turns into established. Greater levels of spondylolisthesis sometimes trigger sciatica, spinal stenosis or cauda equina syndrome. Symptoms are sometimes bilateral with pain, weakness and generally paraesthesiae within the buttocks, thighs and legs. Forward flexion increases the canal diameter and may lead to the adoption of a simian stance. Physical examination is normally unremarkable, and extreme neurological deficits are not often seen. Most circumstances end result from involvement of the spine by metastatic carcinoma (especially prostate, lung, breast, thyroid or kidney) or a quantity of myeloma. A historical past of cancer, unexplained weight reduction and older age are related to a higher likelihood for most cancers. Infection Vertebral osteomyelitis may be acute (usually pyogenic) or chronic (pyogenic, fungal or granulomatous). It normally results from hematogenous seeding, direct inoculation on the time of surgical procedure or contiguous unfold from adjacent delicate tissue. Vertebral osteomyelitis could also be sophisticated by an epidural or paravertebral abscess. Assessment A main focus of the analysis is to determine the few sufferers with an underlying systemic disease (infection, neoplasm or spondyloarthritis) or important neurological involvement (Box 4. It is essential to take a full historical past and carry out a complete physical examination. It is characterized by morning stiffness of greater than half-hour duration, enchancment in back ache with train however not with rest, awakening due to again pain in the course of the second half of the night time, and Physical examination this hardly ever results in a selected analysis. Structural scoliosis is secondary to structural changes of the vertebral column, usually the results of degenerative modifications. Functional scoliosis is often the end result of paravertebral muscle spasm or leg length discrepancy. Functional scoliosis disappears with spinal flexion, whereas structural scoliosis persists. Point tenderness on percussion over the spine has sensitivity however not specificity for vertebral osteomyelitis. A palpable stepoff between adjacent spinous processes indicates spondylolisthesis. Examine the hip for arthritis: this usually causes groin ache and infrequently referred again ache. This take a look at places pressure on the sciatic nerve and stretches the sciatic nerve roots (L4, L5, S1, S2 and S3). Patients with present nerve root irritation, similar to impingement from a herniated disc, will expertise radicular ache that extends under the knee. This test could be very sensitive (95%) but not particular (40%) for clinically significant disc herniation on the L4�5 or L5�S1 stage. Patients may have leftsided sciatica within the distribution of the S1 dermatome and may develop left plantar flexion weak point, diminished gentle touch and pinprick sensation over the lateral side of the left foot, and a diminished or absent left ankle jerk. A major drawback with all imaging research is that most of the anatomical abnormalities (often the results of agerelated degenerative changes) are widespread in asymptomatic folks. Treatment Most patients, regardless of the trigger, respond to a common programme that features analgesia, training, again workout routines, aerobic conditioning and weight control. Examination normally reveals paravertebral muscle spasm and extreme lower in range of motion secondary to pain. Once the acute episode of pain has subsided, a programme of regular back workout routines (including stretching), aerobic conditioning and loss of excess weight is used to forestall recurrences. Flexion workout routines strengthen the belly muscular tissues and extension exercises the paraspinal muscular tissues. Educational booklets that embody back exercises and secure lifting techniques are helpful. There is limited evidence supporting the use of epidural glucocorticoid injections for shortterm aid of radicular pain. Nerve root blocks and injection of anaesthetic brokers or glucocorticoid into trigger factors, ligaments, sacroiliac joints and side joints are of unproven efficacy. Low Back Pain 29 Ultrasound, shortwave diathermy, transcutaneous electrical nerve stimulation and different treatments similar to lumbar braces, traction, acupuncture and biofeedback are ineffective. Lowdose tricyclic antidepressants and serotoninnorepinephrine reuptake inhibitors could assist some sufferers. A multidisciplinary method focusing on useful restoration via an individualized intensive rehabilitation programme based mostly on cognitive behavioural therapy is commonly useful in patients with more intractable ache. Elective surgery is considered for the few with persistent and severe sciatica that fails to respond to conservative care. Surgery is indicated for the presence of a extreme or progressive neurological deficit. Epidural glucocorticoid injections are ineffective in the therapy of spinal stenosis. Surgical remedy, geared toward decompression of the neural elements, is obtainable to sufferers with both disabling, pseudoclaudication or vital neurological deficit. Rarely, a patient might have decompressive surgical procedure with fusion if a big or progressive neurological deficit develops. Unexplained thigh or knee ache ought to, nonetheless, increase the suspicion of hip abnormalities. All babies are screened by physical examination within the neonatal interval, although that is unreliable at detecting many instances. The precise cause is unclear, however the condition is associated with a optimistic household history, low birth weight and lower socioeconomic teams. Treatment aims are to comprise the femoral head in the acetabulum to scale back the dangers of future osteoarthritis. Surgical stabilization to repair the slipped epiphysis in situ ought to be carried out urgently. The contralateral hip is at high threat of slippage, and sufferers and fogeys must be warned to return if any hip or knee pain happens on the unoperated side. Septic arthritis this is relatively unusual in children, however should be suspected if a baby presents with systemic sickness, toxic and inability to walk. Diagnosis is helped by a raised white cell count, erythrocyte sedimentation fee and Creactive protein. An effusion may be seen on ultrasound, and pressing aspiration will help with diagnosis. Staphylococcus aureus is often the infecting organism, however prognosis may be significantly difficult in neonates.
Prevacid 30 mg cheap fast delivery
We have beforehand reviewed the anatomy and historical past of this artery gastritis symptoms upper abdomen purchase prevacid 15 mg otc, which was described by Johann Otto Leonhardt Heubner (1843-1926) gastritis diet jokes 15 mg prevacid buy visa, a German pediatrician, in 1872. The artery of Heubner supplies the anterior striatum (caudate nucleus and putamen), a portion of the outer phase of the globus pallidus, and the anterior limb of the interior capsule. Injury additionally causes dysfunction of the tongue and palate, which can be documented only during a cautious swallowing analysis. In most patients, these deficits are probably to resolve fully in a matter of months. Anatomy of the anterior circulation with the major branches and perforators of the internal carotid artery, of the M1 phase of the middle cerebral artery, of the A1 and A2 segments of the anterior cerebral artery, and of the anterior speaking artery. Most think about it the pericallosal artery, with the callosomarginal as a department of the pericallosal, whereas others use the time period to outline one of many two branches on the bifurcation of the distal A1 section, the opposite department being the callosomarginal artery. The second definition leads to confusion when the callosomarginal artery is absent, as is the case 18% of the time, thus creating ambiguity as to the place the pericallosal artery begins. It originates from the A2 phase in solely 10% of cases and from the A4 section in 12% of circumstances. These important branches provide the optic chiasm, anterior hypothalamus, medial portion of the anterior commissure, pillars of the fornix, and anterior-inferior portion of the striatum (caudate nucleus and putamen). Perlmutter and Rhoton5 reported a range of zero to 4 perforators in their research of 50 brains. Anatomy of the subfrontal gyri and sulci in relation to the course of the olfactory nerve. Yaargil notes that the lateral boundary of the lamina terminalis cistern is a thickened band of arachnoid fibers that stretch between the realm instantly medial to the olfactory nerve and the optic nerve. Importantly, the artery of Heubner and the orbitofrontal artery originate within the lamina terminalis cistern. Anterior communicating artery aneurysms originate throughout the lamina terminalis cistern. Arachnoid Cisterns of the A1 Segment�Anterior Communicating Artery�A2 Segment Region the sequential recognition and opening of three arachnoid cisterns. The A1 phase originates within the carotid cistern before coursing throughout the lamina terminalis cistern over both the optic chiasm (70% of the time) or the optic nerve (30% of the time). Therefore, a clear understanding of the anatomic boundaries of this cistern is essential. This might be so as a result of the upper hydrodynamic pressures generated by the dominant A1 segment drive the growth of the aneurysm. By distinction, inferior-pointing aneurysms are the worst on this respect because elevation of the frontal lobes can avulse the dome from the optic chiasm, optic nerves, or the dura of the interoptic area early within the subarachnoid dissection. Anterior-pointing aneurysms have the most favorable orientation in relation to the hypothalamic and infundibular perforators, and posterior-pointing aneurysms have the worst orientation on this respect. For this reason, anterior-pointing aneurysms are often easier to clip, and posteriorpointing ones are normally essentially the most troublesome. Brain rest is obtained with a Mannitol infusion, mild hyperventilation, drainage of the arachnoid cisterns, and fenestration of the lamina terminalis. Choice of the Side of the Craniotomy We method the aneurysm from the side of the dominant A1 section. When the A1 segments are of equal diameter, we advocate a right (nondominant) craniotomy. This head place allows the frontal lobes to fall away from the cranium base and facilitates the microsurgical exposure. However, this approach has the disadvantage of requiring early retraction of the ipsilateral frontal lobe, which might decompress the aneurysm dome earlier than identification of the paired A2 segments. This incision is more aesthetic than one placed anteriorly alongside the edge of the hairline. Dissection of the Temporalis Muscle A subfascial dissection can be utilized as described by Yaargil and colleagues. This technique protects the frontal department of the facial nerve, which runs along the surface of this superficial temporalis fascia. The incision is started a couple of millimeters anterior to the tragus on the upper border of the root of the zygoma and extended superiorly to the linea temporalis. The anterior frontal bur gap should be roughly 2 cm off the midline in the midpupillary line and as low on the brow as the pores and skin flap permits. The keyhole bur hole must be positioned inferior to the linea temporalis and posterior to the frontozygomatic process to preserve the aesthetically important contours of those prominences. This stretch crosses the frontosphenoidal and the temporosphenoidal sutures and encompasses the lateral side of the larger wing of the sphenoid bone and the anterior-inferior portion of the squamous portion of the temporal bone, simply superior to the root of the zygoma. The fourth bur gap is made beneath the linea temporalis barely on the coronal plane of the temporal bur gap. The fifth posterior frontotemporal hole is positioned equidistant from the two adjacent bur holes. After the bone flap is eliminated, the edge of the remaining temporosquamosal bone is removed with a Leksell rongeur starting above the root of the zygoma and proceeding anteriorly till the larger wing of the sphenoid is encountered. This cumbersome, pyramidal structure gradually leads to a more slender construction, which is the lesser wing of the sphenoid. This is drilled till the dural sleeve of the superior orbital fissure is reached. Removal of these bony buildings allows for a tangential method to the circle of Willis alongside the posterior curve of the lesser wing of the sphenoid. The orbital roof and inside table of the frontal bone are also drilled at this stage. It is necessary not to drill via the orbital roof into the periorbita as a result of this technical error invariably leads to a swollen, ecchymotic eye. If the frontal sinus is entered, it must be exenterated, packed with muscle, and sealed with fibrin glue. Before replacing the bone flap toward the top of the process, a pedicled galeal graft is mirrored over the opening into the sinus, sutured to the dura, and pinched in place between the sides of the bone flap and frontal ledge. The dura is opened in a curvilinear trend from the medial fringe of the craniotomy in the frontal region to the lateral edge of the craniotomy within the temporal region and mirrored anteriorly. Three sutures are then positioned over the region of the sphenoid wing, the anterior fossa ledge, and the middle fossa ledge to retract the base of the dural flap, which in any other case may impede the view along the cranium base. Sutures are positioned over the region of the sphenoid wing, the anterior fossa ledge and the center fossa ledge to retract the bottom of the dural flap, which would otherwise impede the view alongside the cranium base. Freeing the anterior frontal lobe from the burden of the temporal lobe allows for simpler retraction of the frontal lobe. The sylvian fissure is on common 6 cm lengthy and can be divided into three 2-cm parts. Following opening of the fissure in its middle third for roughly 5 mm, the tip of a microirrigation gadget could be inserted into this opening to allow for insufflation of the cistern. The sylvian cistern consists of each a shallow superficial part and a more capacious deep part. These two cisterns are separated by the approximation of the pia arachnoid of the frontal and temporal opercula.
Syndromes
- Sources of protein hydrolysates
- If ejaculation occurs with a broken condom, insert a spermicidal foam or jelly to help reduce the risk of pregnancy or passing an STD. You can also contact your health care provider or pharmacy about emergency contraception ("morning-after pills").
- Foods: Foods passed through breast milk may affect your child. If you are breastfeeding, avoid stimulants such as caffeine and chocolate. Try to avoid dairy products and nuts for a few weeks, as these may be causing allergic reactions in the baby. People often hear that breastfeeding moms should avoid broccoli, cabbage, beans, and other gas-producing foods. However, there is not much evidence that these foods are a factor.
- Intestinal infection
- Did the episode end with a sudden deep snorting breath?
- Vomits more than once
Purchase prevacid 15 mg
The symptom is a uninteresting ache alongside the affected metatarsal shaft gastritis diet �� 30 mg prevacid discount, which modifications to a pointy ache just behind the metatarsal head chronic gastritis lead to cancer prevacid 30 mg generic. Treatment � Rest and local immobilization are often sufficient; the usage of an Aircast boot allows mobilization during this era and is normally required for 6 weeks. Acute synovitis this condition is generally associated with acute trauma, which leads to irritation of the synovial membrane and effusion. Clinical options � It is rare in children however typically impacts younger adults in puberty. The affected person could have skilled trauma or an infection or have a systemic inflammatory disorder. Fusiform swelling is current around the distended joint, and crepitus may be felt. Previously unsuspected systemic arthritis, corresponding to psoriatic arthritis, ought to be investigated. Clinical options � Patients current with a burning or throbbing ache localized to the gentle tissues anterior to the metatarsal heads. The pain normally develops over a couple of weeks, is often associated with strolling in a selected pair of sneakers, and is normally relieved by rest. Direct palpation, rotation and simulation of shear forces on the foot exacerbate the pain. Management � Advice on footwear, with sufficient support or cushioning, ought to be given. Associated abnormal pronation or lesser toe deformities ought to be corrected with orthoses. In the acute type, such as in dancers, squash gamers or skiers, the primary metatarsal is often affected, while the second to fourth metatarsals are predominantly affected in chronic inflammatory arthritis. Clinical features � Patients present with a throbbing ache under a metatarsal head that usually persists at rest and is exacerbated when the world is first loaded. If a superficial bursa is affected there shall be signs of acute irritation, with fluctuant swelling and heat. Direct pressure or compression produces ache, as does dorsiflexion of the related digit. Treatment � Antiinflammatory medication are helpful; in follow, local gels and systemic oral medication assist. Patients must rest the affected half; this may be achieved by immobilization of the forefoot (rockersoled shoe or Aircast). Any underlying deformity or foot type with irregular operate must be assessed and treated. Other circumstances embody true plantar fasciitis, which is characterized by a thickened plantar fascia, and plantar fibromatosis, which is characterised by fibrous nodules and contracture of the fascia. Treatment of true plantar fascial strain requires rest and management of abnormal operate with orthoses, and stretching workout routines. Ultrasound remedy seems helpful and injections of corticosteroid into a thickened plantar fascia seem beneficial, however managed trials are missing. Pain along the medial longitudinal arch Pain alongside the medial longitudinal arch is quite common. Most affected sufferers have irregular foot mechanics, similar to irregular pronation, valgus heel or a flat foot. Tenderness is seen over the decrease posterior part of the tuberosity of the calcaneus. Treatment � In most circumstances, reassurance and advice about lowering actions will suffice: the condition usually subsides spontaneously. In some cases, heel lifts assist; occasionally, if the pain is severe, an Aircast walker boot is needed. Clinical options � A generalized warm uninteresting throbbing pain is felt over the weightbearing area of the heel; this develops over a number of months. Footwear ought to be addressed: a suitably tight heel cap to maintain the heel pad in place beneath the heel, and with shockabsorbing soles. Plantar calcaneal bursitis this is inflammation of the adventitious bursa beneath the plantar aspect of the calcaneal tuberosities. Clinical features � the situation is characterised by an increasingly severe burning, aching and throbbing pain on the plantar surface of the heel. Stretching workouts such as rolling a bottle underneath the foot and calf stretches may help. Little evidence helps ultrasound therapy, native steroid injections or shortwave diathermy. Achilles tendon affections Inflammation of the Achilles tendon and surrounding delicate tissue could also be related to overuse or systemic inflammatory issues (Box 7. Inflammation of the tendon, peritendon tissues and bursae give barely totally different medical footage. Conditions corresponding to xanthoma can also affect the Achilles tendon and produce fusiform swelling within the tendon. In such cases, cholesterol concentrations ought to be checked and treated if raised. Rheumatoid nodules, and infrequently gouty tophi, can additionally be found within the substance of the Achilles tendon Treatment depends on the primary trigger. Partial or full ruptures of the tendon want immobilization and surgical repair. For inflammatory circumstances, nonsteroidal antiinflammatory medicine might assist, as may ultrasound treatment, friction, relaxation and shock absorbing heel lifts. Inflammation could additionally be triggered by overuse by way of poor foot mechanics; in such cases, orthoses may control pronation, if present. Ultrasound imaging could additionally be useful each as a diagnostic tool and to help intervention. Osteochondritis Osteochondritis is an aseptic necrosis or epiphyseal infraction associated with trauma and localized minute thrombosis of the epiphysis. Chronic inflammation of the heel pad this can be a distinct clinical condition that usually outcomes from trauma (jumping) or heavy heel strike. It typically is seen in aged individuals as their fats pads atrophy or in those who abruptly become extra active. Pain is often situated within the center third of the tendon; pain and stiffness are worse very first thing in the morning; ache is normally felt after train however may occur throughout exercise. Biomechanical elements are often concerned within the improvement of degenerative joint modifications. Trauma, recurrent irritation and the calls for of trend footwear such as excessive heels and pointed toes could play an element.

Prevacid 30 mg generic on-line
Experience and end result with postmortem cerebral angiography performed as routine procedure of the autopsy gastritis esophagitis diet prevacid 15 mg order mastercard. Unruptured intracranial aneurysms: pure historical past gastritis pronounce prevacid 15 mg discount on-line, clinical outcome, and risks of surgical and endovascular therapy. Morphological and medical threat elements for posterior speaking artery aneurysm rupture. Recovery of third nerve palsy after endovascular treatment of posterior speaking artery aneurysms. Intraoperative angiography in cerebral aneurysm surgery: A prospective examine of 100 craniotomies. Preoperative predictive value of the need for anterior clinoidectomy in posterior communicating artery aneurysm clipping. Microsurgical anatomy of the cisternal anterior choroidal artery with particular emphasis on the preoptic and postoptic subdivisions. Surgical therapy of 127 anterior choroidal artery aneurysms: a cohort examine of resultant ischemic issues. The keyhole idea in aneurysm surgery-a comparative examine: keyhole versus commonplace craniotomy. The A4 and A5 segments run over the physique of the corpus callosum, with the transition between the 2 segments delineated arbitrarily at the degree of the coronal suture. Duplication of the A1 phase, one other uncommon however surgically necessary anatomic variant occurred in 2% of circumstances, and is unilateral. Unlike the A1 perforators, the majority (51%) terminate within the suprachiasmatic area, with only 15% reaching the anterior perforated substance. The most tough portion of the fissure to open is the horizontal portion in its anterior third in front of the limen insula. With inferiorly projecting aneurysms, a purely subfrontal strategy with preliminary retraction on the frontal lobe can outcome in a dome avulsion and catastrophic hemorrhage too early within the publicity. Furthermore, it is essential to recognize that there may be retrograde circulate through the A2 segments when the A1 segments are occluded, reinforcing the significance of distal and proximal management. Once the origin of the ipsilateral A1 section is reached, the dissection is sustained to free the segment from the inferior surface of the frontal lobe. The medial striate artery of Heubner is identified either anterior or superior to the A1 phase. Care ought to be taken to keep away from inadvertent clipping of the medial striate artery of Heubner with the temporary clip. The contralateral A1 section is then dissected towards the interhemispheric fissure, and the midportion is cleared to enable for momentary clip placement. In cases of inferiorly or anteriorly projecting aneurysm, it might be prudent to place a brief lived clip on the ipsilateral A1 section earlier than initiating the contralateral dissection to expose the contralateral A1 phase, as these aneurysms have a tendency to rupture with even slight retraction. In these situations, as quickly as the contralateral A1 section is identified and its short-term clip is applied, the momentary clip on the ipsilateral A1 section is removed. The pia of the gyrus rectus, immediately parallel and medial to the olfactory, nerve is cauterized. The imply arterial pressure is elevated 10% above the baseline, and burst suppression is initiated. After dissecting the ipsilateral A1 phase and making ready its midportion for short-term clipping, the contralateral A1 phase is uncovered. The ipsilateral opening of the chiasmatic cistern is extended over the anterior fringe of the optic chiasm and over the distal contralateral optic nerve by following the anterior curve of the optic chiasm. The contralateral A1 phase is then dissected distally toward the interhemispheric fissure. At this level, burst-suppression is initiated and, if acceptable, a quick lived clip is utilized to the ipsilateral A1 phase. Using the suction and the bipolar cautery simultaneously, the gyrus rectus resection is quickly completed till the medial pia arachnoid of the gyrus rectus is recognized draped over the aneurysm and the ipsilateral A1 and A2 segments. The ipsilateral medial striate artery of Heubner and the orbitofrontal artery are recognized. For superiorly projecting aneurysms, the contralateral A1 phase could be uncovered, and the distal course of the contralateral medial striate artery of Heubner can be identified, but the contralateral A2 segment is normally hidden. For inferiorly projecting aneurysm, the contralateral A2 segment and origin of the contralateral medial striate artery of Heubner can be uncovered, but the contralateral A1 segment is usually hidden and will should be traced backward, following the course of the A2 section from distal to proximal. Posteriorly projecting aneurysms can obstruct the view of the contralateral A2 segment. Anteriorly projecting aneurysms can partially obstruct the contralateral A1 or A2 section. Regardless of aneurysm orientation, further sharp dissection of the neck and mobilization of the aneurysm are typically required for visualization of the vessels initially hidden from view. The A2 segments often enter the interhemispheric fissure, one anterior to the other and oriented within the sagittal airplane. It can be commonplace that after software of the initial clip, the body and fundus of the aneurysm have to be reshaped with the bipolar forceps (aneurysmoplasty), and even a part of the dome has to be resected to then fully examine the complex. This inspection usually reveals the want to reposition the clip or to apply a second or third clip. The posterior wall of their neck is usually intimately associated with the infundibular and hypothalamic perforators, which must be cleared and displaced below the path of the clip blade. Not infrequently, superior-pointing aneurysms have a further complicating function, which is that one or both A2 segments could additionally be densely adherent to the physique of the aneurysm. Occlusion or damage to these perforators can lead to dramatic neurologic, endocrine, or cognitive deficits. Small orbitofrontal and frontopolar arteries may be sacrificed, however preservation of the medial striate arteries of Heubner is essential. Dissection of the Aneurysm Neck Early dissection of the aneurysm neck differs depending on the projection of the dome. By distinction, inferiorly projecting aneurysms have the disadvantage of usually being adherent to the optic chiasm, optic nerves, or interoptic space, but have the benefit of a more favorable relation to the hypothalamic and infundibular perforators. Similarly, the dome of anterior projecting aneurysms could also be adherent to the gyrus rectus and may rupture during early subfrontal retraction. It is also commonplace that, either earlier than or after application of the preliminary clip, the body and fundus of the aneurysm have to be reshaped with the bipolar forceps (aneurysmoplasty) and part of the dome must be resected (after clip placement) to then totally examine the complicated. This inspection typically reveals the necessity to reposition the clip or apply a second or third clip. If an aneurysmoplasty with the bipolar cautery is attempted, care ought to be taken to rehydrate the sac with irrigation, wax the information of the bipolar forceps to prevent sticking, and reduce the bipolar present to as low as attainable and then improve it as essential until it begins to shrink the wall. Anteriorly projecting aneurysms have essentially the most favorable anatomy on this respect as a outcome of the important infundibular and hypothalamic perforators course in a path reverse the aneurysm. A complicating function of anteriorly projecting aneurysms, however, is that always either the orbitofrontal or a proximal frontopolar artery is adherent to the wall of the aneurysm and should even need to be sacrificed in the course of the clipping. A complicating function of inferiorly projecting aneurysms is that they usually have infundibular and hypothalamic perforators which might be adherent to the posterior aneurysmal wall.
Prevacid 15 mg cheap with visa
Extension of a primarily putaminal hemorrhage into the remainder of the basal ganglia gastritis upper right back pain prevacid 15 mg buy cheap on line, inner capsule gastritis baby prevacid 15 mg buy fast delivery, thalamus, and ventricle was evident at post-mortem. A 77-year-old woman after the acute onset of left-sided weak spot, headache, nausea, and vomiting. Computed tomography showed a right-sided superficial frontoparietal lobar hemorrhage. Neurological examination revealed a neurologically awake and alert patient with strength of 2 of 5 on the left facet. The affected person was treated with medical administration, and her left-sided motor examination findings had improved barely at the time of discharge. Additional presenting signs are variable and dependent primarily on the volume of the hemorrhage. Continued growth of the hematoma will end in a contralateral progressive hemiparesis, hemisensory loss, homonymous hemianopsia, and forced gaze deviation to the facet of the lesion. Hemorrhages in the dominant hemisphere could cause aphasia, whereas nondominant lesions could result in hemineglect. Comatose patients have a poor prognosis, and restoration of neurological perform is unlikely owing to dissection of the deep white matter tracts. Headache is the primary symptom, with neurological deficits varying depending on hematoma dimension and the direction of hematoma dissection via the parenchyma. Lateral extension into the inner capsule or superior dissection into the corona radiata ends in contralateral hemiparesis. Hematoma rupture medially into the ventricular system may obstruct cerebrospinal fluid circulation and result in hydrocephalus. Inferior extension into the midbrain results in devastating neurological damage, together with hemiparesis and doubtlessly coma. Chronic abuse of intravenous medicine, together with heroin, can also result in vasculitic adjustments, vessel wall weakening, and rupture. Headache, nausea, and vomiting are the initial signs, that are followed by disorientation. This medium-sized hypertensive thalamic hemorrhage, which spared the capsular fibers laterally, is well confined. Dissection of the hematoma into the thalamus results in transient short-term memory deficits. These hemorrhages are most frequently found within the subcortical white matter of the parietal, temporal, and occipital lobes, which accounts for the decrease incidence of coma and stuck neurological deficits. This intensive hypertensive cerebellar hemisphere hematoma started within the deep nuclei and extended. The time course over which symptoms manifest is variable, and rapid deterioration into coma and even dying can happen without warning. In common, those with hematomas larger than three cm are more probably to quickly deteriorate, develop obstructive hydrocephalus, and require emergent surgical evacuation. Extension of the hematoma into the encompassing white matter could dissect into the fourth ventricle and lead to obstructive hydrocephalus. Symptom onset follows a progressive course beginning with dizziness, neck stiffness, and dysarthria. Further deterioration consists of appendicular and truncal ataxia, peripheral facial palsy, ipsilateral sixth nerve palsy, and nystagmus. If no surgical intervention happens, sufferers with sizable hematomas will turn out to be increasingly much less responsive. At the time of presentation to a hospital, approximately one third of patients are comatose. Neurological examination reveals focal pontine signs, similar to diplopia, hemiparesis or quadriparesis, sensory deficits, and probably deafness. Many of these patients will survive with varying persistent neurological deficits. Large hematomas end in coma with decorticate or decerebrate posturing, irregular respiration patterns, pinpoint pupils, and ocular bobbing. While en path to the hospital, he turned progressively extra lethargic and was not arousable on admission. Computed tomography demonstrated a 6-cm right-sided cerebellar hematoma with compression of the fourth ventricle. An emergent suboccipital craniectomy and hematoma evacuation have been performed (B and C). The affected person was discharged to a rehabilitation facility ambulating with assistance. Chronic speaking hydrocephalus requires ventriculoperitoneal shunting after the clot resolves. Regardless of whether the affected person is treated with surgical evacuation, medical management plays a crucial role in figuring out end result. As outcome, a complete strategy should be taken to the care of this complicated patient population, which is most likely finest carried out in a neurological intensive care unit. Suri and colleagues demonstrated that aggressive blood pressure discount was protected and probably useful within the first 24 hours after admission. The American Heart Association/American Stroke Association guidelines suggest the continual infusion of labetalol, nicardipine, esmolol, or other antihypertensive brokers to achieve a goal blood stress based on the presenting blood stress. Patients develop a giant number of comorbidities, in several age groups, and with varied neurological examination findings; blood stress ought to be managed with these variables in mind. The median admission glucose within the demise group was 205 mg/dL versus 131 mg/dL in the survivors. Further statistical analysis discovered an admission blood glucose of 150 mg/dL to be the cutoff value for predicting early dying. Diabetes was an unbiased predictor of 30-day and 3-month mortality in noncomatose sufferers. Nondiabetics with hyperglycemia additionally had poorer outcomes and a higher incidence of cerebral complications. Emerging information additionally counsel that aggressive glucose management with an insulin infusion can result in a low cerebral extracellular glucose focus. These objectives maintain true even in sufferers on systemic anticoagulation for thrombotic states with a threat of ischemic problems. Warfarin is probably the most frequently encountered systemic anticoagulant and is often used for thromboembolism prevention in patients with situations similar to mechanical heart valves and atrial fibrillation. Multiple brokers are at present employed within the reversal of warfarin-induced coagulopathy; however, no consensus has been reached in figuring out the optimum regimen. Intravenous vitamin K has a sluggish onset, taking approximately 6 hours to obtain therapeutic ranges. Conversely, these brokers also carry the danger of a probably greater incidence of thromboembolic issues. If neurosurgical intervention is required, sufficient reversal may be reliably achieved only with hemodialysis, causing probably life-threatening delays. Future studies are required to better perceive the function of these agents, the true danger of neurological issues, and the neurosurgical administration of such hemorrhages. Lobar hemorrhage, most probably brought on by the shut proximity to the cortical surface, was considerably associated with the occurrence of early seizures.
Order 15 mg prevacid with amex
Axial and coronal T2-weighted (A and B) and sagittal T1-weighted (C) magnetic resonance images show multiple vascular circulate voids within a left frontal arteriovenous malformation extending from the cortex right down to gastritis and stress 30 mg prevacid free shipping the frontal horn of the left lateral ventricle gastritis pictures prevacid 15 mg discount visa. Left inner carotid injection (lateral projection) during cerebral angiography shows that the arterial provide is by way of anterior left middle cerebral artery branches (D) with early venous drainage (E). Bleeding is typically from rupture of a draining vein, associated with dilation, kinking, and thrombosis, or from rupture of flow-related aneurysms, that are extra prevalent than in adults. Histologic section shows that the partitions of the veins are thickened and hyalinized and often lack elastic tissue and clean muscle. The surrounding mind parenchyma reveals evidence of previous microhemorrhage, hemosiderin staining, and hemosiderin-laden macrophages. Although several case stories have implicated capillary telangiectasias as a explanation for hemorrhage, this has been proved histopathologically only in a few instances. Asymptomatic lesions are recognized Pathology, Pathogenesis, and Pathophysiology the vessels of a capillary telangiectasia are enlarged or dilated, which units them aside pathologically from normal cerebral capillaries. They are often small (<2 cm in diameter) and largely solitary (78%) and may have an result on any area of the mind. The pons is the most typical location, adopted by the middle cerebellar peduncle and the dentate nucleus of the cerebellum. Mild gliosis can surround the parenchyma, but hemosiderin and other proof of prior hemorrhage are uncommon. A, Computed tomographic scan of the mind of a 50-year-old man with acute intraventricular and pontine hemorrhage. B, Digital subtraction angiography exhibits a posterior fossa arteriovenous malformation supplied by the left posterior inferior cerebellar artery and superior cerebellar vermian branches with fast arteriovenous shunting into the torcula and left transverse sinus. An associated developmental venous anomaly is seen in the lateral (C) and anteroposterior (D) projections. Axial T2-weighted (A) and contrast-enhanced T1-weighted (B) magnetic resonance pictures in a 25-year-old with a sudden onset of headache, diplopia, and dizziness show recent hemorrhage into a pontine cavernoma. Central hemorrhagic merchandise are surrounded by a partial hemosiderin rim, and an related developmental venous anomaly can be famous (arrow). The answer at current is unknown, and any theories will ultimately be proved or disproved by histochemical analysis. Garner and coworkers reported one such patient,fifty nine and Awad and coworkers reported three. Mullan and colleagues reviewed four such patients and discussed the pathophysiology in the context of embryologic growth of the cerebral venous system. This finding may indicate that some sufferers have respectable hypertension and disruption of the blood-brain barrier,56 which is indicated by contrast enhancement. Recognition of familial clustering in a subset of sufferers with cerebrovascular malformations has led to linkage analysis research investigating the underlying genetic basis for these lesions. This means that a genetic defect underlies at least some vascular malformations. In addition to enhancing presymptomatic screening, identification of the genes responsible might result in higher understanding of the pathogenesis of those lesions and, in the end, in novel therapies. Nasal, mucocutaneous, pulmonary, cerebral, gastrointestinal, and hepatic vascular beds are most commonly affected. E, Funduscopy shows multiple dilated and tortuous retinal vessels, findings confirming the diagnosis of Wyburn-Mason syndrome. Knockout mice lacking endoglin die during gestation because of faulty vascular growth, suggesting that endoglin is crucial for vascular development. No mutant endoglin was expressed on the cell floor, however somewhat it was discovered only as an intracellular homodimer. They exhibit vascular abnormalities, together with hyperdilation of vessels and abnormal fusion of capillary structures. Isolated familial predisposition in the absence of an angiodysplastic syndrome is exceedingly rare. Some authors have advised an autosomal dominant mode of transmission with variable penetrance95-97 or an X-linked recessive pattern of inheritance. To date, the involvement of genetic factors in such nonhereditary syndromes has not been clearly demonstrated. The first intraembryonic angioblasts appear at the single-somite stage (during the third week of embryonic life), and interconnection with their extraembryonic counterparts is established on the two-somite stage. Advances in our understanding of angiogenesis and vascular reworking have supplied new insight into the pathophysiology of vascular malformations in the brain, and consequently, potential new remedy methods are emerging. Feeding arteries and draining veins are typically mature, normal-appearing vessels, which can have some degree of wall thickening. This concept of active angiogenesis and vascular transforming in intracranial vascular malformations is opening a brand new medical paradigm in which pharmacologic interventions are proposed to stabilize these abnormal blood vessels and forestall further progress or hemorrhage. Research on intracranial vascular malformations has been specializing in identifying roles of angiogenic and antiangiogenic factors in their pathophysiology. Such changes can trigger vascular remodeling, the process of which can further have an effect on native hemodynamics. Whether acquired or congenital, ongoing vascular remodeling and angiogenesis, presumably triggered by aberrant local hemodynamics, have been thought of to be a critical component of their pathophysiology. This increased move ends in cerebral arterial hypotension along the path of the shunt. Despite vital cerebral arterial hypotension, most patients are free from ischemic signs. Hypotensive normal brain areas could be demonstrated, for essentially the most part, to have comparatively regular levels of tissue perfusion, implying some adaptive change in complete cerebrovascular resistance. A evaluation of the studies that examined interval angiograms from a total of 106 patients with mean follow-up time of eight. Angiogenesis and vascular remodeling are managed by the orchestration of numerous angiogenesis-related factors. The residual nidus grew and recruited new feeding vessels and was excised surgically. Angiopoietin and Tie-2 Angiopoietins and their receptor, Tie-2, play a critical position in angiogenesis and vascular stability. Ang-1 and Ang-2 are both approximately 75-kD secreted proteins with appreciable sequence homology; both bind to Tie-2 with similar affinity, and neither binds to Tie-1. Ang-1 is widely expressed in embryos and adults, whereas Ang-2 seems to be current in tissues present process active vascular remodeling, such as the ovary, uterus, and placenta. Ang-2 competitively inhibits the Ang-1-induced kinase activity of Tie-2 and functions as an Ang-1 antagonist. It has been advised that Ang-2 could have a more biologically lively role than simply being an antagonist in opposition to Ang-1.
Real Experiences: Customer Reviews on Prevacid
Ramirez, 22 years: Chahlavi and colleagues107 reported two instances by which the AngioJet was used successfully with direct transcranial puncture. It runs in a lateral course, which makes it readily seen from the lateral facet, and it can be duplicate or, in rare circumstances, triplicate. In explicit, we suggest aggressive management of hypertension, prompt institution of calcium channel blockers. The craniotomy should be approximately 6 cm in rostrocaudal size and 5 cm in width, extending 2 cm contralaterally across the sagittal sinus.
Spike, 46 years: Small residual dog-ears may be observed; nevertheless, cautious long-term follow-up is essential. EndovascularFlowDiversionfor 393 IntracranialAneurysms Alexander Drofa, Gabor Toth, Peter Rasmussen, and Mark Bain Before the introduction of endovascular flow-diverting units, the term flow diversion was typically used along side cerebrovascular neurosurgical procedures. The authors attributed this comparatively excessive fee of mortality to both poor scientific grade or postoperative ischemia from vasospasm. Seizures enhance cerebral oxygen consumption and should cause hypoxemia, hypercarbia, acidosis, aspiration, and pneumonia.
Wilson, 36 years: After barbiturates are administered, short-term clips are placed on every pericallosal artery just past the genu of the corpus callosum. The lesions, in short, when accidentally exposed by the surgeon had higher be left alone. It is often graded as delicate (<25%), reasonable (25%-50%), or extreme (>50%) in comparability to baseline, prevasospasm imaging. Cervical myelopathy (compression of the spinal cord), which may come up as a outcome of midline disc herniation, is recommended by a historical past of difficulty in strolling and bladder and bowel dysfunction.
8 of 10 - Review by R. Murat
Votes: 300 votes
Total customer reviews: 300
