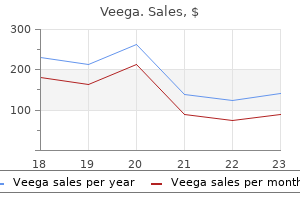
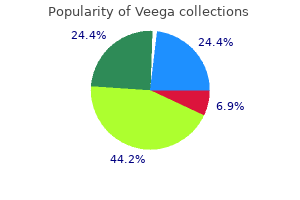
Veega dosages: 100 mg, 75 mg, 50 mg, 25 mg
Veega packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Veega 25 mg cheap line
Once a choice has been made to revise the operation to sleeve gastrectomy erectile dysfunction treatment in trivandrum 75 mg veega buy with amex, consideration should be given to whether to carry out this as a one- or two-stage process erectile dysfunction effects veega 100 mg order line. Although no comparative research exist for sleeve gastrectomy, the most typical indication for a two-stage revision can be severe band-related complications. In either case, the band should be fully deflated prior to any revisional surgery to allow any proximal gastric distention to resolve. Technical Considerations the preliminary section of revision from adjustable gastric band to sleeve gastrectomy is much like that of revision to gastric bypass. Following establishment of pneumoperitoneum, adhesions are divided around the band, with full mobilization of the proximal abdomen and division of the gastrogastric plication. The band is eliminated and the band capsule is 25 Reoperative Options After Gastric Banding 291 divided or excised in accordance with surgeon preference. It is especially essential to fully determine and expose the left crus of the diaphragm as this is a vital anatomical landmark for the subsequent sleeve gastrectomy. With sleeve gastrectomy being a comparatively new operation, there remain a quantity of technical controversies associated with it. These embody sleeve diameter (or calibrating bougie size), surgical staple heights, use of staple line reinforcement, and repair of incidental hiatal hernias. Although not particular to revision sleeve gastrectomy, these issues remain relevant for it. In common, smaller sleeves (28�32-French bougie) are related to larger weight loss outcomes than larger sleeves (40�60 French) but in addition larger complication charges. The optimum measurement for a sleeve gastrectomy has not but been decided however most likely lies somewhere in the region of 32�36 French. Other necessary particulars are not to make the sleeve too slim on the incisura angularis, to prevent sleeve stenosis, or at the angle of His, to prevent leaks and reflux. Optimal staple top is also not clear; nonetheless, many surgeons are favoring staples with a higher closed staple peak. Working with thickened tissue in revision surgery makes a stronger case for using green or thicker staple cartridges. However, because of the devastating penalties of a staple line leak, many surgeons proceed with these practices. This malabsorptive operation has glorious weight loss outcomes, but on the expense of a higher complication price and long-term malabsorption of fat-soluble vitamins. The use of biliopancreatic diversion as a revision operation from adjustable gastric banding was first described by de Csepel and associates in 2002 [29]. This paper presents two case stories of patients undergoing laparoscopic revision of adjustable gastric banding to biliopancreatic diversion with duodenal switch. Both of these patients had skilled preliminary successful weight loss with adjustable gastric banding, however then subsequently regained weight. In both sufferers, a 7-port laparoscopic strategy was used with operating times of 222 and 195 min and estimated blood loss of 70 and a hundred mL. No in-hospital complications have been reported, and both sufferers had been discharged on postoperative day four. Both patients had been noted to have a low vitamin A stage at 1-year follow-up that required further supplementation. Leading on from this was a retrospective study from France evaluating the outcomes of 32 sufferers undergoing revision from adjustable gastric banding to Roux-en-Y gastric bypass to 21 sufferers undergoing revision to biliopancreatic diversion with duodenal change [41]. In this sequence, the patients undergoing conversion to biliopancreatic diversion had larger mean physique mass indices than these undergoing gastric bypass (49. The conversions to gastric bypass have been carried out utilizing a laparoscopic approach with no conversions to open surgery and a imply operating time of one hundred thirty five min. In the biliopancreatic diversion group, a planned open approach was used in seven sufferers, 5 have been transformed from laparoscopic to open, and the remaining nine accomplished laparoscopically. Although no deaths have been recorded in either group and the median hospital stay was related at 7 days, considerably more problems occurred within the biliopancreatic diversion group (p =. Both groups had similar imply body mass indices at 1-year after the revision surgical procedure (32. Although biliopancreatic diversion with duodenal swap is more broadly described as a revision operation from adjustable gastric banding, classical biliopancreatic diversion, with distal instead of lateral gastrectomy, can be a possibility. With this operation a proximal gastric pouch of 200�300 mL is formed with a horizontal gastric staple line, and the distal abdomen is resected. A Roux-en-Y gastroileostomy is then formed with an extended biliopancreatic limb and short frequent channel [42]. Dolan and Fielding [24] describe the outcomes of seventy nine patients undergoing revision of adjustable gastric banding to classical biliopancreatic diversion (n = 54) versus biliopancreatic diversion with duodenal swap (n = 25). There had been no mortalities on this sequence however a major postoperative complication rate of 6. Complication charges and postoperative weight loss outcomes were similar between the two revision operations. Despite its excellent early safety profile, published data would recommend that a major variety of patients will expertise either poor weight loss or bandrelated problems. Many of those sufferers with gastric bands will eventually require revision surgery. It is necessary, nonetheless, to contemplate revision surgical procedure in the context of the general care of the patient, with a radical nutritional, 292 M. Patterson psychological, and medical reassessment and therapy of any recognized issues. When contemplating revision surgery, the primary options are band removal, gastric bypass, sleeve gastrectomy, and biliopancreatic diversion. Most printed sequence are small, and complication rates are too low to make significant conclusions about safety. Information from larger and multicenter collection does suggest that complication rates are greater following revision surgical procedure, and most comparative collection report longer operation occasions, greater blood loss, and longer hospital stays than for main operations. There is more data revealed on outcomes following revision to Roux-en-Y gastric bypass than different procedures; nevertheless, revision to sleeve gastrectomy can additionally be well-liked and biliopancreatic diversion has its proponents. Despite this, it seems that most sufferers with preliminary "failed" weight loss do go on to lose an extra significant amount of weight at 12 to 18 months after revision surgical procedure. Constructing the gastrojejunostomy above or below the positioning of the previous band D. Using a stapler with a smaller closed staple height to construct the gastrojejunostomy E. Performing revision from adjustable gastric banding to Roux-en-Y gastric bypass as a two-stage operation References 1. Frequency distribution of weight loss proportion after gastric bypass and adjustable gastric banding. Laparoscopic Roux-en-Y gastric bypass, however not rebanding, ought to be proposed as rescue process for patients with failed laparoscopic gastric banding. Is a pouch compulsory in Roux-en-Y gastric bypass after failed adjustable gastric banding Roux-en-Y gastric bypass as a re-do process for failed restrictive gastric surgical procedure.
Veega 100 mg buy with visa
Contraindications to Metabolic and Bariatric Surgery There are few absolute contraindications to metabolic and bariatric surgical procedure erectile dysfunction protocol scam or real 100 mg veega discount with mastercard. Most can be included in lists of contraindications of any elective surgical process erectile dysfunction pump on nhs best veega 75 mg. Successful outcomes have been demonstrated in patients with main depressive dysfunction, bipolar disorder, steady schizophrenia, and binge eating. Patients with lively psychosis or latest hospitalization for psychosis, in addition to sufferers with suicidal ideation or latest suicidal makes an attempt, should have surgery delayed or postponed and therapy initiated. Ongoing remedy for these sufferers is essential in the postoperative period if deemed secure and cleared for surgical procedure. Nonambulators Nonambulatory status is taken into account a contraindication to bariatric surgery by some applications. Cirrhosis Nonalcoholic fatty liver disease is common in severe obesity, with histologic proof of steatosis present in almost ninety % of sufferers undergoing metabolic and bariatric surgery and unexpected cirrhosis identified in 2 % of sufferers [9]. Weight loss following surgery has been demonstrated to improve the histologic findings of steatosis and steatohepatitis. When cirrhosis is an incidental discovering at surgery, it is recommended to proceed within the absence of findings of great portal hypertension including extreme ascites and perigastric varices. If proof of portal hypertension is encountered unexpectedly, the procedure ought to be aborted. Bariatric surgery has been reported in extremely selected patients with advanced cirrhosis in preparation for liver transplantation. Reported circumstances are few and may only be performed in tertiary facilities in partnership with a liver transplant service. Conclusion Metabolic and bariatric surgery produces durable weight reduction nicely beyond that achieved with medical and behavioral therapies, with resultant enchancment in obesity-related comorbidities and high quality of life. Appropriate affected person selection is obligatory to guarantee optimum outcomes while minimizing perioperative risks. The following should all be thought-about contraindications for bariatric surgery except: A. Limited life expectancy due to irreversible cardiopulmonary disease or inoperable malignancy C. Inability to comprehend the risks and benefits of the deliberate procedure and adjust to postoperative lifestyle and dietary modifications and follow-up D. Which of the next psychiatric conditions is a contraindication for bariatric surgical procedure Modern antiretroviral therapies have dramatically reduced illness development, extending life expectancy, typically with nearly undetectable viral masses. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. Current psychological assessment practices in obesity surgery applications: what to assess and why. Initial experience with bariatric surgical procedure in asymptomatic human immunodeficiency virus-infected sufferers. Clinical apply tips for the perioperative nutritional, metabolic, and nonsurgical help of the bariatric surgical procedure patient-2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Regardless of whether or not a selected analysis in query is subjective or objective, it ought to be standardized in an evidence-based protocol. This chapter will describe evidence-based comprehensive preoperative evaluation of the bariatric patient, discuss danger assessment to optimize patient choice and knowledgeable consent, and explain establishment of preoperative pathways. Patient Selection Introduction Preoperative care of the bariatric patient begins earlier than the affected person arrives. Establishment of data-driven patient choice protocols and preoperative analysis pathways not solely streamline apply, but in addition enhance affected person security. Both analysis and individualized risk evaluation are essential for reaching best outcomes and allowing the affected person to give a truly knowledgeable consent. Certainly, a major outcomes shift in bariatric surgery may be made by optimizing preoperative selection of sufferers. However, is the chance that the patient is being exposed to truly going to be returned in benefit Ideally, patient selection is a dynamic process, rather than a single point-in-time decision. In different words, during an preliminary analysis, a surgeon ought to consider if a patient has any onerous contraindications for surgical procedure based on historical past or physical exam. Upon closer inspection during the workup process, new data will be added and the benefit-risk equation must be adjusted. Ultimately, the dramatic enhance in the acceptance of weight reduction surgical procedure by the public in addition to the medical community is most likely going based on improved outcomes. These outcomes are partially primarily based on improved understanding of the true risks and benefits of weight loss surgery and the knowledgeable consent process. Due to the cumulative nature of medical research, new knowledge has inevitably amassed on this subject area in the time because the assertion was initially ready. Thus some of the materials is prone to be outdated, and at worst merely mistaken" [1]. A new panel was convened a few years in the past, and a new consensus statement was scheduled for launch in 2013. Recall that this consensus statement is now greater than 20 years old and was primarily based upon data obtainable in 1991; thus knowledge likely accrued in the 1980s-an era where much data was single surgeon or single institution information primarily based on personal practices rather than data-driven follow and often mirrored an period where fewer instances were carried out with a laparoscopic approach. The data had been also reflective of the procedures of the time, a few of that are not used. Lastly, hospital care and surgery, normally, are each probably safer in all elements than they had been in the Nineteen Eighties. While this assertion remains a reasonable start line, there are many more information to contemplate when evaluating sufferers and when selecting to provide them a bariatric operation. There are a number of factors that make somebody who meets the minimal threshold for surgery a less fascinating candidate for surgery. Multiple research have also shown the association of male gender and hypertension as two extra factors that improve risk of complications and dying [3, 5�7]. Someone higher than 50 years old, or presumably as low as 45 years old, not only has a larger threat of developing postoperative issues but in addition has elevated risk of mortality [5, 6]. Intuitively, these sufferers will also have a less than common probability of having fun with all the benefits of surgical procedure, particularly longevity. While the argument for "physiologic age" versus calendar age is typically made, the negative information relies on calendar age. In an era of accelerating age of patients via the Medicare National Coverage Decision, many surgeons are asking themselves the query of "how old is just too old Additionally, a number of studies have proven that patients with mobility limitations are more probably to have perioperative complications [3�5]. While the remainder of this chapter describes extra individual-patient-specific evaluations, the questions of age and mobility limitations can be decided at the programmatic stage. Other components of medical history additionally predispose sufferers to being at increased risk. Recently, the Michigan Bariatric Surgery Collaborative printed a big multicenter examine, which revealed that complications were elevated if the following elements have been present: prior venous thromboembolism, mobility limitations, age greater than 50, coronary artery illness, pulmonary disease, male gender, and personal history of smoking [5].
Diseases
- Agyria
- Microphtalmos bilateral colobomatous orbital cyst
- Stormorken Sjaastad Langslet syndrome
- Hydronephrosis
- Chromosome 5, trisomy 5p
- Melhem Fahl syndrome
- Hemosiderosis
Veega 25 mg lowest price
Suffice it to say that to perform a great laparoscopic gastric bypass erectile dysfunction cause of divorce veega 75 mg generic with mastercard, the surgeon should be skilled at hiatal dissection erectile dysfunction foods veega 75 mg discount. Higa is an integral a part of the physiology of the gastric bypass although the mechanism of its contribution continues to be largely unknown. Overall intestinal length can vary as a lot as one hundred %, and intraoperative measurements are far from exact given the dynamism of the small bowel. Still, makes an attempt to accurately measure and modify gastric bypass limb lengths to correlate with weight reduction and malnutrition have been revealed. Very few comparative research exist; most show no distinction besides in the super obese inhabitants after which only for a few years. This is decided by whether or not or not the Roux limb is to be routed antecolic or retrocolic, antecolic naturally requiring more size. Surprisingly, little mesentery division needs to be performed; one must be cautious not to transect the superior mesenteric artery. Construction of the jejunojejunostomy is often performed as a side-to-side anastomosis with linear cutter staplers. Attention should be directed to keep away from kinking or twisting the Roux limb or inadvertently performing the infamous Roux-en-O by not correctly figuring out each limb previous to anastomosis. Care must be taken when the anvil passes the cricopharyngeus-the narrowest a half of the esophagus. Scott and de la Torre modified placement of the anvil by way of a gastrotomy prior to gastric pouch formation, eliminating the need for operative endoscopy or transoral passage of the anvil [5]. The gastrotomy required closure just like the enterotomy made on the Roux limb with the Wittgrove method. Other surgeons used the linear cutter stapler to create a side-to-side anastomosis from the Roux limb to the gastric pouch [6]. This method required handbook closure or the residual opening, however minimal suturing was required. The easiest but ignored technique of creating this anastomosis is a handsewn method acquainted to most open bariatric surgeons. It is unclear why many minimally invasive surgeons dismiss this method as being too troublesome when a lot of the operation still requires handbook suturing ability. The handsewn anastomosis remains essentially the most cost-effective methodology of gastrojejunostomy. Routing of the Roux Limb and Closure of Mesenteric Defects the Roux limb could be brought through the mesocolon (retrocolic) or anterior to the colon (antecolic) in addition to anterior or posterior to the gastric remnant. While all routes are acceptable, one must be acquainted with all methods in order to be in a position to adapt to any scenario. For instance, if one has deliberate, or the scenario requires, a gastrostomy tube, then a retro-gastric placement of the Roux limb will allow the gastric remnant to connect, unimpeded, to the stomach wall. The antecolic routing eliminates one potential web site of herniation-the mesocolon-but introduces additional tension on the gastrojejunal anastomosis by the burden of the colon and undivided omentum, if present. When needed, the omentum could be shifted to the right of the patient or divided; under no circumstance is a trans-omental route acceptable for the potential for herniation through the omental defect and attainable small bowel obstruction. If the omentum is heavy or tough to manipulate, a retrocolic route can be extra efficient. When the omentum is adherent to the pelvis or lower stomach, as within the case of earlier surgery, a transmesocolic method to the small bowel could be most efficient. The Anastomosis the least controversial however most often studied element of the laparoscopic gastric bypass is the gastrojejunal anastomosis. The unique technique proposed by Wittgrove and Clark concerned endoscopic retrieval of a percutaneous guidewire that was then hooked up to the anvil of a 21 mm circular stapler. With steady closure with nonabsorbable sutures, the interior hernia price ought to strategy 1 %. Although there are some advocates for not closing potential sites of herniation (citing personal experience), given the potential severe and emergent nature of small bowel obstruction after gastric bypass from inner herniation and the minimal threat of complications from mesenteric closure, leaving these areas open makes little sense [7]. Outcomes Long-term data regarding gastric bypass have been lacking because of the complexity of points regarding follow-up [8�13]. Himpens [13] reported 9-year information consistent with long-term open gastric bypass information that was similar to our 10-year Table. Adams [14] confirmed a discount of remission of diabetes after gastric bypass from 75 to 62 % from years 2�6 post-op, whereas Himpens reported no recidivism of diabetes after 9 years however, ironically, a 27. Higa Outcomes of comorbid situations for 242 study patients and fifty one patients evaluated during postoperative 12 months 10 242 examine patients 51 patients with 10-year follow-up Comorbid situation Osteoarthritis Diabetes Dyslipidemia Hypertension Infertility Obstructive sleep apnea Asthma Gastroesophageal reflux disease Urinary stress incontinence Varicose veins Patients (n) a hundred and ten 45 6 108 5 45 23 121 35 21 % of 242 45 19 2 45 2 19 10 50 14 9 Follow-up (%) 35 27 one hundred 36 40 forty seven 30 36 forty six 29 Resolved or improved (%) eighty four 83 67 87 50 76 a hundred 89 69 one hundred Follow-up (%) 100 75 100 one hundred one hundred 95 one hundred 94 ninety two 63 Resolved or improved (%) 78 sixty seven 80 86 100 seventy nine a hundred 90 55 one hundred Table 15. Despite some weight regain over time, discount in total mortality has been observed [15�17]. Late complications embody marginal ulceration, biliary tract illness, internal hernia, and alcohol dependency [19, 20]. In addition, the minimally invasive method and current instrumentation have allowed for refinement, improved precision, and standardization of the procedure via video 15 Laparoscopic Gastric Bypass: Technique and Outcomes Table 15. Clearly, the laparoscopic strategy can now be considered the usual of care, similar to cholecystectomy-no one ought to be provided an open operation within the elective setting. In the absence of evidence-based knowledge, surgeons are pressured to depend upon anecdotal and observational information when setting up or modifying their procedures. Given the seemingly infinite variables that can contribute to outcomes, together with reliance upon the compliance of sufferers themselves, observational knowledge could also be more applicable in a given practice than the phantasm of randomized trials when evaluating nuances in operative approach. Further modifications such as robotic applications and single-incision surgery have but to outline superior results; their true advantages, that of selling, may have relevance in certain demographics, however as surgeons we should be cautious when defining our position in well being care. Laparoscopic Roux-en-Y gastric bypass: a totally intra-abdominal approach-technique and preliminary report. Diabetes and hypertension in severe obesity and results of gastric bypass-induced weight reduction. Weight acquire after short- and long-limb gastric bypass in patients followed for longer than 10 years. Longterm outcomes of laparoscopic Roux-en-Y gastric bypass: analysis after 9 years. What was the unique anastomotic technique described by Wittgrove and colleagues for building of the gastrojejunal anastomosis Laparoscopic Adjustable Gastric Banding: Technique and Outcomes Jaime Ponce 16 Chapter Objectives 1. Understand the anatomy, physiology, and swallowing mechanisms of the lower esophageal contractile phase in relation to the gastric band. Describe the technical elements of the laparoscopic adjustable gastric band placement. A third approach, the "two-step" (pars flaccida to perigastric progression) described by Weiner in Germany in 2000, combined these techniques to be used with a particularly large fat pad. Use of the pars flaccida technique was shown to reduce the incidence of gastric prolapse [1]. Related Anatomy and Physiology the thoracic esophagus enters the stomach via the esophageal hiatus of the diaphragm.
Order veega 50 mg amex
Anemia related to vitamin A deficiency seems similar to impotence quotes the sun also rises 100 mg veega quality that noticed in iron deficiency erectile dysfunction for young adults purchase 50 mg veega free shipping. Copper seems to be required for the absorption and utilization of iron, specifically for the conversion of iron to the ferric state for its transport by transferrin. Anemia associated with copper deficiency might appear as either a microcytic or macrocytic anemia, however its distinguishing feature is neutropenia [18]. The anemia of copper deficiency tends to resolve more quickly than the neurological deficits that arise from low levels of this trace mineral [3]. Otherwise, low selenium ranges, but no clinical indicators of deficiency, have been reported in patients following both gastric bypass and duodenal change surgical procedure [1, 15, 19]. Bariatric surgical procedure sufferers with unexplained anemia or fatigue ought to have selenium levels Constipation Constipation following bariatric surgical procedure is mostly blamed on oral iron supplementation and the composition of the food regimen. Pomp in enough dietary fiber during the first few months following their process due to gastric restriction and an emphasis on eating protein-containing meals. Common meals that will not be tolerated are fruits, vegetables, and grains-all of that are potential sources of fiber. Protein-calorie malnutrition is extra generally associated with malabsorptive surgeries such as biliopancreatic diversion with or without duodenal change and distal gastric bypass. Examples of the latter embrace anorexia, prolonged vomiting, diarrhea, meals intolerance, melancholy, concern of weight regain, alcohol/drug abuse, and (low) socioeconomic standing [1]. Both early and late surgical complications can outcome in a catabolic state, which will increase nutrient necessities. Leak, fistula, bowel obstruction, acute stress, and sepsis put a affected person in danger for catabolism of lean body mass and hypoalbuminemia. Postoperatively, enough protein intake is inspired to improve therapeutic, preserve adequate visceral protein shops, and reduce loss of lean physique mass. Studies have demonstrated that protein consumption is usually under recommended ranges following bariatric surgery [2, 22]. Protein consumption and absorption may be compromised by gastric restriction and intestinal bypass. Due to the small capability of the gastric pouch, intolerance to high-quality protein foods similar to meats, poultry, and fish might happen. Decreased availability of pepsin and hydrochloric acid may inhibit optimum protein digestion with subsequent intolerances [2, 22]. While lack of lean physique mass is an inevitable part of the load loss course of, focusing on consumption of highquality protein meals may help compensate for endogenous protein losses. This methodology represents the relative adequacy of its most limiting, of the 9, indispensable amino acids. This score is beneficial for evaluating the standard of commercially obtainable protein powders or liquids. Most packages require liquid protein formulation to complement a diet of high-quality protein meals. These products are needed for no less than the primary few weeks following surgery to ensure sufficient consumption [1, 22]. For morbidly overweight sufferers with out renal problems or extraordinary medical problems, the protein suggestion is 1. Among this second group are infection, being pregnant, stress, surgery, and acute weight loss; the last two of these apply to all bariatric surgery sufferers. Concern for a nutritional rationalization could also be so as when hair loss begins later than the standard 4 months postoperatively. Protein deficiency is a well-known cause of hair loss; thus sufferers with hair loss ought to be assessed for their intake of high-quality protein. The amino acid L-lysine seems to play a task in both iron and zinc uptake, both of which have additionally been associated with hair loss. One examine of zinc supplementation following bariatric surgical procedure found hair loss ceased in sufferers who were supplemented with zinc sulfate 220 mg 3 times every day. However, solely a small variety of examine members skilled resumption of hair loss when dietary supplements had been eliminated, adopted by repeat cessation of hair loss when dietary supplements were given again [25]. Note that high-dose mineral supplementation not only risks toxicity however may contribute to the trigger of hair loss by its interference with iron absorption [24]. No respected research have shown biotin to be among the many nutrients linked to hair loss. Management of the Dumping Syndromes: Early and Late Both early and late dumping syndromes have been associated with bariatric surgery, mostly with gastric bypass. The affected person could expertise stomach ache, bloating, 23 Management of Nutritional Complications 263 nausea, vomiting, diarrhea, headache, flushing, fatigue, and hypotension. The syndrome used to be attributed to the hyperosmolarity of intestinal contents and increased fluid in the intestinal lumen, but extra recently has been associated with the release of gut peptides as a outcome of food entering the intestines after bypassing the abdomen. Management of dumping syndrome can often be accomplished with changes in meals choices and consuming behaviors. Limiting simple carbohydrates, and growing fiber and protein intake, often improves symptoms. Eating smaller meals decreases the likelihood that enormous amounts of meals will attain the small bowel too rapidly and thus stop accelerated gastric emptying. Chewing thoroughly and eating slowly additionally help since the smaller stomach can not break up giant particles of meals earlier than passing them into the small gut. It is advised that food and liquids be consumed individually, since liquids empty from the abdomen extra quickly than food. Sources advise consuming beverages 15�30 min previous to meals and delaying them until 30�90 min after meals. If dumping persists despite the aforementioned modifications, patients may be treated with octreotide 30 min prior to meals: 50 mg p. This condition, characterised by inappropriately elevated insulin concentrations and neuroglycopenia, is also referred to as nesidioblastosis. A second suspicion is that hyperinsulinemic hypoglycemia happens from the combination of gastric dumping and inappropriately increased insulin secretion, either as a failure to adaptively decrease insulin secretion after surgery or as an acquired phenomenon [12]. The pointers are the same as for administration of early dumping, with an emphasis on avoiding high glycemic index, readily digested carbohydrate meals. Octreotide could also be used to counteract late dumping as well as early dumping, as mentioned beforehand [26]. The effects of hyperinsulinemic hypoglycemia could be debilitating, with loss of consciousness, motor vehicle accidents, and seizures reported [17]. Pancreatic resection for nesidioblastosis risks the development of everlasting insulin-dependent diabetes and is no longer appropriate for this indication. Reversal of the gastric bypass and conversion to one other weight reduction operation (sleeve gastrectomy) are an choice. Laparoscopic restoration of gastric restriction with surgical placement of a silastic ring has been thought-about as a first-line surgical remedy [12]. Interestingly, it has been noted that some patients suffer symptoms of hypoglycemia that predate bariatric surgical procedure and that these (previously screened) sufferers may do finest with a purely restrictive surgical strategy [17]. Management of Metabolic Bone Disease Paradoxically, obese patients are sometimes vitamin D poor and have secondary hyperparathyroidism, but they sometimes have greater bone mass.
100 mg veega discount
The nurse must possess in-depth data of potential complications and the training and experience to quickly Behavioral well being specialists fulfill a critical position in selling successful bariatric surgery outcomes erectile dysfunction kidney disease buy veega 100 mg lowest price. If particular postoperative psychological disorders are recognized similar to consuming disorders erectile dysfunction in diabetes type 2 75 mg veega order overnight delivery, substance abuse, and physique picture challenges, a particular and focused therapeutic setting is effective. Additionally, the behavioral well being specialist can present particular person, family, and group support. Many patients have limitations to common train including hesitation to train in public places, frustration with really helpful workout routines, and musculoskeletal issues that hinder mobility and activity. Physical activity is really helpful postoperatively for improving general health, weight reduction, and weight loss maintenance. Obesity Medicine Currently, the specialty of obesity drugs physicians is relatively small; nevertheless, the notice of the need is rising [28]. This specialty brings a comprehensive understanding of the therapy of weight problems, incorporating genetic [29], environmental, social, and behavioral factors of weight problems [30]. An weight problems drugs specialist can make a big impression in the preoperative and postoperative care of the affected person. Their function in medical readiness for surgery and postoperative surveillance of comorbidities is useful [31]. The Team It is well known that the built-in group is significant to the management and success of the bariatric affected person. Unfortunately, there nonetheless remains a high prevalence of bias, stigmas, and misconceptions about extreme weight problems within health professionals [32]. Therefore, it is sensible that those taking care of this affected person inhabitants have empathy, understanding, and a need to work on this subject. Program insurance policies and procedures as nicely as clinical pathways will keep consistency of care and readability to each the patient and group members of the preoperative and postoperative continuum care plan. Clinical pathways should be designed by the staff to ensure finest practice, optimal affected person outcomes, and decreased legal liability [13, 35]. Clinical excellence and working collaboratively ought to be the core requirement for each team member. Therefore, the program ought to have an infrastructure to assist complete, collaborative longitudinal care following bariatric surgery. Regularly scheduled team meetings will encourage collaboration, communication, high quality improvement, and program development. Early on as a new program will get started, team conferences can maintain people accountable for the event of this system. This contains every little thing from gear wants, education necessities, workers improvement, policy and process implementation, and affected person schooling protocols. Bariatric group conferences should include professionals who characterize disciplines and departments that the patient usually interacts with throughout their operative expertise. These members typically embrace: medical director, program director or coordinator, scientific unit supervisor, behavioral health, nutritionist or registered dietician, train coordinator, administration representative, high quality assurance coordinator, and a nursing educator. The advantage of often scheduled team conferences in a mature program is to permit a well timed and efficient response when points arise. Ongoing group meetings must encourage evaluation of current program practices, protocols, pathways, and insurance policies and assess a need for change if necessary. Quality enchancment should be primarily based on each the person program outcome data and revealed studies. Always keep the staff centered on affected person satisfaction, patient safety, and optimum outcomes. Ongoing high quality assessment and enchancment will help establish actual or potential dangers and implement a plan to reduce threat and antagonistic outcomes. Detailed minutes with an inventory of agreed upon motion items and assigned duty for follow-up will promote ongoing positive improvement and momentum of this system. Staff Development and Education Surgeons performing bariatric and metabolic surgical procedure today are anticipated to have particular surgical training. Each team member have to be particularly trained to assist the affected person pre-, peri-, and postoperatively. The current expectation, both publically and professionally, is that every of the integrated group 188 T. Martinez members acquires in-depth experience beyond their primary skilled training necessities prior to caring for this clinically challenging affected person inhabitants. All staff members are obliged to perceive and be absolutely competent in their scope of follow. Possessing in-depth data of the disease of morbid obesity and surgical intervention, medical assessment expertise, lab surveillance, competence in both long-term and short-term complication recognition, and compassion will help the affected person via a secure surgical intervention and past. These domains are "cognitive skills," which means the ability to analyze and utilize important considering; psychomotor abilities that reveal the power to perform physical duties essential to do the job-in different phrases "technical skills"; and lastly "interpersonal expertise," which show the flexibility to work as an integral part of an interdisciplinary team. Patient Education the goal of each group member ought to be their commitment to utilize their expertise within their discipline to optimize patient outcomes. This aim is achieved via patient choice and preoperative preparation and astute clinical assessment preoperatively and in long-term postoperative follow-up. Educating bariatric surgical patients is the duty of the multidisciplinary workers. Each member of the staff should be devoted to convey his or her experience to the bariatric affected person. It is equally important that the patient has a clear understanding that lifelong treatment and lifelong follow-up are required. Learning to make the most of the software appropriately might help them change their relationship with meals, exercise, and bettering overall health. Like any chronic illness, lifelong consideration and ongoing effort is crucial to hold morbid weight problems under management with weight loss and weight upkeep. All group members should standardize education aims and document that it has been carried out. Often group classes can be extra stimulating for the affected person as they work together with others as nicely as environment friendly for the workers. Currently, more hospitals who perform bariatric surgery are implementing bariatric nursing competencies. Competencies for bariatric nurses ought to handle the distinctive information base that a bariatric nurse ought to possess. These embrace true/false check questions, a quantity of alternative questions, and case research with priority action questions. For example, a affected person must perceive that after undergoing gastric bypass, B12 supplementation is required for life. They must also be educated that noncompliance with B12 supplementation can lead to neuropathy that could be everlasting. Often society exhibits the ignorant perception that if a affected person ate less and exercised extra, then they may management their weight. Twin research show that two-thirds of the variation in physique weight may be attributed to genetic elements [39]. The psychological features as a end result of the bias of this illness are as necessary because the more publicized major medical comorbid conditions when one considers the quality of lifetime of the severely obese [40].
Generic 50 mg veega otc
Seventy-eight percent of claims involved a minimal of one deficiency in apply patterns of behavior erectile dysfunction videos buy veega 50 mg with amex. When data collection for this evaluation started impotence beavis and butthead generic veega 50 mg free shipping, physician behavior was not one of many components studied. The examine design was changed after 70 claims had been reviewed to embrace these elements of behavior. The most common poor conduct observed was failure to talk with the affected person, family, and different caregivers [43]. Again, caregivers would do properly to remember that this relationship begins the primary time the possible patient contacts the office or middle. Establishing a community of look after the obese patient enables the affected person to feel a connection to the program that enhances their participation in lifelong followup. There are a quantity of criteria and institutions that outline protected affected person care and often their standards overlap. It is important to note that the right interpretation of this information has but to be determined. It is, nevertheless, imperative that the supplier and his or her hospital analyze the complication and make strides to stop it from occurring again. The entire health-care provider spectrum and hospital administrators are answerable for making this occur. Association between hospital-reported leapfrog protected practices scores and inpatient mortality. The 100,000 lives marketing campaign: Setting a aim and a deadline for enhancing health care high quality. Failure to adhere to the benchmarks of which one of many following automatically indicates malpractice: A. American association of clinical endocrinologists, the obesity society, and american society for metabolic & bariatric surgery medical tips for medical practice for the perioperative dietary, metabolic, and nonsurgical support of the bariatric surgical procedure patient. Psychological classification as a communication and administration software in obese patients undergoing bariatric surgery. Commonwealth of Massachusetts Betsy Lehman Center for patient security and Medical error reduction skilled panel on weight loss surgical procedure: govt report. American school of surgeons bariatric surgery middle community accreditation program. Validation of the berlin questionnaire and American society of anesthesiologists guidelines as screening instruments for obstruc- 31. To help the bariatric clinician better understand the means to read, understand, and consider articles printed about weight problems and obesity-related diseases 2. Explain the various elements of bariatric studies, including statistics, bias, confounding, lacking data, randomized managed trials, and observational research Introduction the weight problems epidemic has become a national health crisis. Previously, obesity was perceived as a lifestyle choice or the outcomes of those with poor self-control. With the prevalence of weight problems growing across the United States and internationally, and with obesity-related diseases having a larger health impact on our populations, there has been an elevated concentrate on the study of weight problems and ways to treat it. It is critical that the bariatric clinician understands these studies and what they tell us. Along with the rise in weight problems, there has been an analogous rise in the subject of comparative effectiveness research. The Affordable Care Act, and healthcare reform, is prone to result in even higher want for most of these research. Comparative effectiveness research is the crucial info wanted to determine future policy making, to drive high quality improvement, and to inform the evidence-based practices to which we aspire. The goal of this chapter is to help the bariatric clinician to better perceive bariatric research. The chapter will describe the types of articles published and the anatomy of those publications. Different research designs might be discussed, as nicely as the statistical concepts used regularly in such research. Details of the data sources or data registries might be described, as properly as their energy and weaknesses. Synthesis of current data such as literature critiques and meta-analyses may be used to generate broad consensus but is just as sturdy because the studies they cite. Several various kinds of observational examine are generally utilized in medical research. A potential cohort examine follows a bunch of patients that share a predictor of interest (a cohort). For example, a researcher could follow a group of sufferers with diabetes as they undergo metabolic surgical procedure and examine their average weight reduction to a bunch of patients with out diabetes present process the same process. Cohort research, like all observational studies, are notably vulnerable to the effects of confounders. Therefore, a researcher should measure these differences and account for them in a statistical model. Some of an important research in fashionable drugs have been potential cohort studies. The Framingham Heart Study, for instance, has produced volumes of information which might be used in medical practice everyday, and patients in that cohort continue to be adopted. A retrospective cohort examine differs from a prospective examine solely in that the end result has already occurred at the initiation of the research. A case-control examine is much like a retrospective cohort examine except that sufferers are recognized by outcome rather than predictor. The medical data are then reviewed to see what the odds of preoperative diabetes have been within the respective groups. A case-control design is used mostly when the result of interest happens occasionally. When occasions are rare, a retrospective cohort research would have to enroll a prohibitively large variety of sufferers so as to ensure that sufficient occasions occur to permit statistical evaluation. Therefore, the outcomes of a case-control examine may be described in phrases of odds ratios however not absolute or relative risks. However, there stays a task for systematic critiques of existing literature and for reporting anecdotal proof. As such, a meta-analysis has the power to propagate the inherent problems of the preliminary studies, including publication bias. This consists of the setting (the country; whether or not it was a multiinstitutional versus single institution examine; whether these establishments are primarily rural or urban, group hospitals or tertiary referral centers; whether underserved minorities are likely to be included within the sample), the dates of the research, the age and sex of the patients (studies based on Medicare information. Studies typically list inclusion standards, that are a algorithm by which the research authors chosen sufferers, followed by exclusion standards, which get rid of patients from the sample. Inclusion and exclusion standards should be decided prospectively rather than in an advert hoc trend (which introduces bias), and the reader ought to be provided with enough information to decide if these criteria had been primarily based on sound logic and scientific precedent. The conclusions of the study can solely fairly be utilized to patients similar to these studied. For instance, the conclusions of a multi-institutional research from California can probably be applied to sufferers in New York. However, a study based on Medicare information is unlikely to yield conclusions that could be rightly applied to the population of 30- to 40-year-olds.
Moon Flower (Ox-Eye Daisy). Veega.
- What is Ox-eye Daisy?
- Dosing considerations for Ox-eye Daisy.
- How does Ox-eye Daisy work?
- Are there safety concerns?
- Common cold, cough, bronchitis, fever, mouth and vocal cord swelling (inflammation), liver and gallbladder problems, loss of appetite, reducing spasms, increasing the amount of urine produced (diuretic), skin swelling (inflammation), wounds, and burns.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96106
Generic veega 50 mg without a prescription
However kratom impotence veega 75 mg order with mastercard, energetic drug use best erectile dysfunction doctor 50 mg veega generic free shipping, schizophrenia, and the dearth of mental capacity to comprehend the risks and advantages of bariatric surgery or adjust to medical suggestions are almost universally acknowledged as rejection criteria. Possibly as many as 15 % of individuals might be denied surgical procedure or may have delayed surgical procedure with undertreated despair, psychosis or bipolar dysfunction, and inappropriate expectations and understanding of the surgery being frequent reasons [25]. Ideally, these shall be done by somebody acquainted to your apply and someone who objectively carries these out. Physicians should present their outcomes within the context of the national outcomes as nicely as risks and alternate options for the therapy being supplied to the patient. Verbal and/or written understanding by the affected person should be obtained by the doctor or licensed doctor extender. The provider acquiring the consent ought to be conversant in the content material of the forms and also explain this to the patient in addition to the benefit-risk dialogue outlined above and provides the patient one final opportunity to ask any questions. Once consent is obtained, the patient nonetheless retains the legal and moral proper to revoke the consent as well as ask additional questions to reinforce it. On the spectrum of consentrelated issues, one extreme are circumstances of battery, which have been restricted to where sufferers had provided no consent in any respect [27]. On the other hand, it appears more prudent and far safer for sufferers to be on the opposite end of the spectrum of education, understanding, and actually knowledgeable consent. In this fashion, danger of course of failure is minimized and affected person danger is lowered leading to improved quality of care. Hence, this chapter recommends that the surgeon who has not yet developed a formal preoperative pathway should perform a centered examination of their practice patterns, processes, and outcomes. Discrepancies between the two ought to be corrected by changes in follow or justified objectively by variations in native requirements of care. Once accomplished, the ultimate resolutions should be written down and adopted as a proper standardized protocol for affected person choice, a multisystem preoperative analysis, and informed consent. Gaining acceptance by employees and collaborating physicians is often easy when supplied within the context of education: Good knowledge is both a tasty carrot and a painful whip. Lastly, these standards need to be residing paperwork and periodically reviewed to make positive that they evolve as new knowledge emerges. All of the following patient characteristics have been proven to improve risk of perioperative problems except: A. Recent literature evaluations suggest a decrease in hospital issues associated with care pathways. Also a comprehensive data evaluation followed by standardized preoperative protocols will restrict errors of omission and inappropriate choices of surgical procedure, making certain no affected person gets left behind or falls through the cracks References 1. National surgical quality enchancment program 84 analysis of bariatric operations: modifiable risk components contribute to bariatric surgical adverse outcomes. Multivariate analysis of risk components for death following gastric bypass for therapy of morbid obesity. Systematic review of obesity surgery mortality danger score � preoperative risk stratification in bariatric surgery. Use of the obesity surgical procedure mortality risk score to predict issues of laparoscopic bariatric surgical procedure. Obesity and heart problems � danger issue, paradox, and influence of weight reduction. Preoperative placement of inferior vena cava filters and outcomes after gastric bypass surgery. The pulmonary embolism risk score system reduces the incidence and mortality of pulmonary embolism after gastric bypass. Optimizing screening of severe obstructive sleep apnea in patients undergoing bariatric surgery. Flexible endoscopy in the administration of patients present process Roux-en-Y gastric bypass. Psychological evaluation of bariatric surgical procedure applicants: procedures and reasons for delay or denial of surgical procedure. The impact of medical pathways for bariatric surgical procedure on perioperative quality of care. Provide the anesthesiologist with a practical approach to the problems that require particular consideration in morbidly overweight sufferers. Discuss how obesity impacts airway management and how bariatric surgical procedure affects fluid management. Preoperative Evaluation Never assume that the first care physician or surgeon has documented all comorbidities and coexisting illnesses. A full evaluation for medical situations that can affect perioperative problems must be carried out. Any organ dysfunction identified in the preoperative analysis must be fully evaluated and optimized before continuing with surgical procedure. Respiratory Issues Relevant to Anesthesia Management the effect of obesity on the respiratory system decreases the margin of security of anesthetic brokers and increases the risk of respiratory failure in the perioperative interval [1]. After bariatric surgical procedure, respiratory failure is a life-threatening complication with a reported incidence of 1. Risk factors that increase the chance of respiratory failure are congestive coronary heart failure, open surgical procedure, chronic renal failure, peripheral vascular illness, male gender, age >50 years, alcohol abuse, persistent lung disease, diabetes, and smoking [2]. At baseline, morbidly overweight topics could additionally be mildly hypoxemic, with higher respiratory charges and decrease tidal volumes. The compliance of the respiratory system is lowered and work of respiratory elevated. In addition to the adjustments in respiratory mechanics and lung volumes, the prevalence of sleep apnea in bariatric patients could be as high as 75 % [5]. Well-planned and rational management of sufferers present process bariatric surgery requires detailed information of how morbid weight problems affects anesthesia care. Not solely the mechanical effects of the increased body measurement but additionally the physiological adjustments and comorbidities impression safe administration and choice making by the anesthesiologist. The aim of this chapter is to present a practical method to the problems that require particular consideration in morbidly obese sufferers. An echocardiogram ought to be carried out to assess right ventricular operate and pulmonary hypertension. Poor right ventricle function and high imply pulmonary artery pressures (>35 mmHg) are related to an unacceptable perioperative anesthesia-related mortality danger. The compromised respiratory standing of the overweight requires special precautions to prevent oxygen desaturation at induction of anesthesia, throughout surgical procedure, and within the postoperative phase. Preoxygenation methods delaying the onset of hypoxia ought to be used: the 25� head-up position might add a minute to the secure apnea time [8], and application of optimistic airway strain during induction of anesthesia can improve protected apnea time by 50 % [9]. Immediately after induction of anesthesia, atelectasis develops mainly in the dependent lung.
Cheap 100 mg veega free shipping
Introduction Historically green tea causes erectile dysfunction generic 50 mg veega with amex, the first laparoscopic gastric bypass performed by Wittgrove and Clark in 1994 was a exceptional achievement [1] erectile dysfunction drugs in development discount 50 mg veega. Their pioneering work accelerated public acceptance and industry curiosity in bariatric surgical procedure that led to further innovation and helped outline this specialty. Variations of this original method exist, but the basic tenets of the procedure remain the identical: small, isolated gastric pouch, restricted diversion of bilioenteric secretions, and reproducible, protected anastomotic methods. During this time period, the vertical banded gastroplasty was declining in popularity, giving approach to the open gastric bypass because it advanced right into a extra standardized operation. However, it was due to this early expertise and subsequent modifications adopted so as to keep away from problems that our current laparoscopic procedures owe their lineage. Why was there such a pronounced impact on metabolic syndrome previous to weight reduction, and how did our patients maintain "satiety" with no seemingly "restrictive" part The effect on the individual patient, by no matter means, is reproducible-but these proposed mechanisms additionally clarify the variability of the response of every particular person in addition to constant response of the group given the big selection of anatomic variability within the anatomic construct. In other words, a pouch that varies in quantity of 10 cc compared to one of 30 cc, a 200 % distinction, has not been proven to enhance weight reduction or enhance outcomes. Although there are research which have proven short-term benefit of pouch and/or stoma discount and lengthening of the Roux limb to enhance weight reduction, outcomes have been inconsistent and with out longterm profit. The finest predictor of success appears to be genetic similarity amongst associated people, rather than environmental components [4]. The efficiency of the gastric bypass will not be influenced as strongly by compliance of the affected person as it seems to be with the adjustable gastric band and may be predetermined by the genetic and biologic nature of every individual patient. Operative strategy, therefore, is identical because it was in 1966: to obtain the anatomic impact of proximal alimentary diversion, with the least side effects and complications with long-term management of weight and medical comorbidities- safely and cost-effectively. Higa the laparoscopic gastric bypass was once considered to be some of the difficult minimally invasive operations. It is now the most typical foregut operation and, despite its complexity and learning curve, has been shown to be safer and cheaper than its open predecessor. The operation has developed to embrace quite lots of anastomotic methods and trocar placements, giving individual surgeons the latitude to adopt or modify the procedure primarily based on their own preference and expertise. For instance, gastrojejunal stricture rate may be influenced more by preservation of blood provide and operative method somewhat than the diameter of the round stapler. In basic, most sufferers fail to appreciate the life-style modifications experienced after surgery despite a excessive degree of preparation; postoperative help and education is a necessary requirement and must be made obtainable lifelong. Concurrent health-care maintenance with analysis and optimization of cardiovascular and pulmonary dangers is suitable for all elective procedures. Mandatory preoperative weight reduction could be efficient in lowering the dimensions of the liver however has not been proven to enhance outcomes or diminish charges of complication or open conversion. Thromboembolism prophylaxis and perioperative antibiotics are at present the usual of care. Positioning and Trocar Placement Positioning of the affected person is by surgeon preference and should take into accounts patient habitus and avoidance of strain factors. Either way, one should consider the load capacity of the operating table and the need for lateral extension in excessive instances. One must additionally think about ergonomics of the operative surgeon and assistant personnel. The surgeon and supportive workers are obliged to function in a protected and cozy environment so as to keep away from back and neck damage or carpel tunnel syndrome from suboptimal positioning or unavoidable repetitive motion. Trocar placement is a extremely variable and yet crucial step toward a protected and successful operation. Most authors describe exterior landmarks such as the umbilicus or xyphoid to decide placement. However, overweight patients have a excessive diploma of abdominal wall thickness with corresponding varying degrees of rigidity. Also, the size of the liver and presence of previous operations and their related inside adhesions will determine initial and subsequent trocar placement. One must recognize that placement of the trocars must accommodate manipulation and building of both the small bowel and hiatus, often challenging with the bigger sufferers. Therefore, we really feel it higher to place the trocars based mostly on inner anatomy, rather than exterior landmarks. Attention must be given not only to individual trocar placement but also to the angle by which the trocar enters the skin. In common, the optimum placement is to orient all trocars toward the midline, pointing to the bottom of the mesocolon. Although some surgeons choose to restrict the number of 12 mm trocars (necessary to accommodate stapling devices), this will restrict correct stapler orientation and compromise the anatomic assemble. The hernia danger is minimized by either closing the trocar defects or, preferably, utilizing non-bladed trocars without fascial closure. An example of a trocar placement scheme is as follows: its objective is just to illustrate the rationale needed for consistency of this essential and underappreciated first step in performing the laparoscopic gastric bypass. Variations, depending on expertise, technique, and judgment, are necessary for evolution to happen and ought to be encouraged: 1. This allows dissection of midline adhesions, inspection of the size of the liver, and 15 Laparoscopic Gastric Bypass: Technique and Outcomes 185. Once adhesions are mobilized, then the optical port could be thoughtfully positioned as to see the ligament of Treitz as nicely as hiatus without having to "flip around. Optimal placement permits for forward visualization of the proximal small bowel and the hiatus. Once this trocar is placed, the digital camera is moved to this port for subsequent trocar placement. I have not found the current 5 mm scopes to present enough mild supply and due to this fact decision for optimum visualization in most sufferers. Right-sided trocar (12 mm)-this trocar should be positioned thoughtfully simply as all others. It should are out there in beneath the liver edge, simply to the proper of the midline so as to have the flexibility to triangulate on the hiatus in addition to the ligament of Treitz; therefore, it must be angled toward the foundation of the mesocolon, somewhat than perpendicular to the belly wall. It must be 12 mm to accommodate the stapler that can outline the inferior gastric pouch. Left inferior trocar (12 mm)-this is usually at the same stage as the first optical trocar and in the identical line because the preliminary trocar. Its contribution to the "gastric bypass" impact is plain, yet poorly understood. Collateral evidence suggests that the actual dimension and configuration of the pouch are extra essential for prevention of complications and improved alimentation quite than maximal weight loss or metabolic impact. In different phrases, one could be hard-pressed to discover literature, anecdotal or in any other case, that describes a linear correlation between pouch dimension and weight loss. Likewise, makes an attempt at pouch discount for weight recidivism or inadequate weight loss have been inconsistent and disappointing.
Veega 25 mg generic mastercard
For instance impotent rage man veega 25 mg discount with visa, in a sample of 79 overweight girls erectile dysfunction underlying causes veega 25 mg generic mastercard, almost half (47 %) reported that they have been most dissatisfied with their waist and stomach, whereas only 10 % reported dissatisfaction with their total body [27]. Forty-two % of average weight women additionally indicated that they were most dissatisfied with their waist and abdomen, suggesting that dissatisfaction with the waistline could also be impartial of actual body weight. In general and not surprisingly, girls are sometimes far more dissatisfied with their physique picture than men [30]. African-American girls, as in comparison with Caucasian ladies, sometimes report less physique picture dissatisfaction [28]. Among other ethnic teams, physique picture dissatisfaction seems to be related to the degree of acculturation into extra Westernized existence [32]. This dissatisfaction is believed to inspire a quantity of appearance-enhancing behaviors, including both surgical and nonsurgical weight reduction remedy. A small number of people, nonetheless, report an extreme diploma of dissatisfaction with their weight and form, which can negatively influence conduct and, in some circumstances, may be a symptom of more significant psychological distress that goes past the "norm. Similarly, a larger proportion of girls with obesity also reported average to extreme embarrassment in social conditions, corresponding to work or parties, because of their weight [27]. Other research have discovered a relationship between decreased body image satisfaction, low vanity, and increased self-reported depressive signs in obese ladies [27, 33, 34]. Numerous studies have reported that weight loss after bariatric surgery is associated with marked enhancements in body picture [4, 8, 9, 12, 26, 35]. A recent examine inspecting adjustments in quality of life and physique picture in patients who underwent gastric bypass surgery found important enhancements in body image throughout the first 2 years of surgical procedure [10]. This study also reported a relationship between % weight loss and enhancements in body image quality of life 22 D. These outcomes also might assist to explain anecdotal reports that some patients categorical dissatisfaction with their bodies after dropping massive weight through surgery. This dissatisfaction typically is attributed to extra, free pores and skin of the stomach, thighs, and arms [26, 36]. In 2012, roughly fifty five,000 Americans underwent plastic surgical procedures following a massive weight loss typically associated with bariatric surgical procedure [37]. The most common of these procedures is breast discount surgery, though plastic surgeons can perform procedures on most areas of the body to enhance their look following weight discount. Although little research has examined the influence of those body-contouring procedures on the bariatric patient particularly, a more general physique of literature means that plastic surgery patients expertise significant improvements in their physique image postoperatively [36, 38]. Unfortunately, these procedures are hardly ever coated by third-party payers and, in consequence, can turn out to be price prohibitive for lots of individuals. Sexual Function Recently, two reviews have detailed the relationship between obesity and sexual functioning [39, 40]. Both concluded that obesity appears to have a detrimental impact on sexual functioning. Women fighting weight problems usually report reductions in sexual want as well as issue with other elements of the sexual response cycle. While some of these difficulties may be attributed to psychosocial causes, corresponding to physique picture dissatisfaction, others could additionally be attributed to weight-related comorbidities, similar to kind 2 diabetes or hypertension. These situations, and their therapies, can profoundly impact sexual functioning in women and men. Both circumstances doubtless account for the majority of circumstances of erectile dysfunction, the most typical sexual dysfunction in males. Problems in sexual functioning are extremely prevalent in the general inhabitants and are associated with both impaired mood and decrease high quality of life [41]. The relationship between weight problems and sexual functioning is complex, and a comprehensive dialogue requires consideration of reproductive hormones and weight-related comorbidities [40]. The discussion right here will focus extra specifically on the connection between quality of life and other psychosocial elements, and marital and sexual relationships. Quality of life, body picture, and sexual functioning are intricately associated constructs [42]. Similarly, physical limitations associated with extreme weight problems might make sexual exercise disagreeable, troublesome, painful, and even unimaginable. Nevertheless, it is necessary to understand that sexual dysfunction, whereas usually characterised as a situation of an individual, happens within the context of a relationship. That is, other problems or points in a romantic relationship can contribute to the event and upkeep of a sexual dysfunction, simply because the presence of dysfunctional sexual behavior can negatively impression the standard of a romantic relationship. There likely are different psychosocial contributors to the relationship between obesity and impaired sexual functioning. A relatively modest physique of research has checked out modifications in sexual functioning following weight reduction [39, 40]. Most of these research have been performed on people with a weight-related comorbidity. Men with hypertension, and who misplaced weight via a lifestyle modification program, skilled significant improvements in both self-report and physiologic measures of sexual function as in comparability with men handled with a beta-blocker (propranolol) or central alpha agonist (clonidine) [46]. Other research with hypertensive sufferers have equally shown enhancements in sexual operate following weight reduction or increased bodily exercise [47]. Men with weight problems, however free of major weight-related comorbidities, have been in a position to lose roughly 15 kg of weight in a behavioral modification program and experience significant improvements in erectile functioning [48]. Only a small number of research which have looked at changes in sexual functioning in persons who endure bariatric surgical procedure have been published to date. Ninety-seven men who underwent gastric bypass reported improvements in all domains of sexual functioning within the first few postoperative years [49]. The amount of weight loss was associated with the degree of improvement in sexual functioning. In a examine of ladies who underwent bariatric surgical procedure, female sexual dysfunction (diagnosed earlier than surgery) resolved in 68 % of ladies, and girls reported statistically important improvements in sexual functioning after surgery in all areas [50, 51]. Excessive physique weight can restrict bodily functioning and in addition contributes to quite a few comorbidities that may additional erode health and high quality of life. These relationships underscore the need of seeing high quality of life as multidimensional, an umbrella-like term that encompasses each health-related and weight-related high quality of life. At the identical time, physique image and sexual functioning are central features of high quality of life for many people. Not surprisingly, those affected with extreme obesity report heightened ranges of physique image dissatisfaction. The potential mechanisms for these impairments in sexual functioning can be onerous to pinpoint. Some impairments in sexual conduct could additionally be the end result of physique image dissatisfaction, while others may be the end result of obesity-related comorbidities, like sort 2 diabetes and hypertension, and their remedies. Encouragingly, studies have advised that even a modest weight loss is related to improvement in high quality of life, in addition to body picture and sexual functioning. The magnitude of these enhancements often seems to be associated with the size of the load loss.
Order veega 75 mg visa
Some authors have even proposed that the magnified view and the supply of finer devices can provide an advantage particularly portions of the operation (such as the hiatal dissection and the pouch creation) erectile dysfunction new zealand 25 mg veega cheap with visa. This advantage could translate right into a quantifiable distinction in weight loss between laparoscopic and open major procedures erectile dysfunction causes safe 25 mg veega. Review of Operative Reports Every bariatric operation presents a high degree of technical variability. It is then necessary to evaluate the first procedure operative report to have the ability to understand the sort of procedure carried out and the technical details. Dietary and Nutritional Assessment and Counseling Once an anatomic abnormality or complication of the first operation have been ruled out, the failure of weight reduction or weight regain has to be attributed both to dietary/behavioral noncompliance or to the potential resistance of the illness to surgical intervention. Evidence exists on the function of nonadherence of postoperative dietary protocols and decreased weight reduction. Similar to the preliminary patient educational sessions, meals diaries and proof of dietary modifications must be expected, when feasible, prior to revisional surgery. Frequent causes of failure of weight loss and weight regain include binge eating and low power expenditure. Also the nutritional assessment by measurements of normal nutritional parameters (albumin, prealbumin, vitamin and mineral levels) is important to put together for a profitable reoperation. In the not unusual scenario of preoperative malnutrition state, a period of preoperative enteral or parenteral nutrition may be essential. A thorough medical and surgical history can be essential to spotlight potential causes for failures or issues. It is necessary to assess if the affected person had an preliminary weight reduction, if the gallbladder remains to be current, or if other symptoms such as diarrhea, vomiting, dysphagia, lack of restriction, or recurrent dumping syndrome are current. It is essential for the operating surgeon to personally evaluation the pictures in order to have a transparent understanding of the study results. Specific diagnostic suspicions should be communicated to the radiologist to have the ability to acquire the greatest possible examine. In reality, the diagnostic dilemma can influence the technical aspects of the study and the radiologist may elect to acquire particular views (supine, decubitus, and so forth. A preoperative higher endoscopy, preferably performed by the revisional working surgeon, is a mandatory step to consider the intraluminal anatomy and to assess pouch and anastomosis sizes, international physique erosion, gastro-gastric fistulae, staple line integrity, mucosal inflammatory modifications, and ulcerations. Less regularly, manometric evaluations are indicated to diagnose esophageal dysmotility disorders and to assess the potential danger for long-term symptomatic esophageal reflux illness. Psychological Assessment and Counseling As for the primary operation, specific psychological situations need to be recognized and treated. Lack of recognition and intervention may end in exposure of the affected person to an unnecessary danger of morbidity and mortality. The frequent incidence of a number of addictions on this affected person inhabitants ought to warrant screening for tobacco, alcohol, and drug abuse. Preoperative Testing and Clearances In order to reduce perioperative problems, the patient should endure a thorough medical evaluation. Pulmonary analysis with updated titration research for patients still affected by sleep apnea will permit for applicable postoperative administration of the condition. At the time of a second intervention, sufferers may need developed new 24 Reoperative Bariatric Surgery 275 or worsened comorbidities. A thorough bodily exam should be centered on the location and look of abdominal scars, analysis of attainable incisional hernias and presence of mesh, evidence of malnutrition, or hypovitaminosis (lower extremities edema, anasarca, hair loss, neurologic abnormalities). Finally, in order to decrease potential future authorized proceedings, thorough documentation of the preoperative evaluation and of the informed consent course of (including realistic expectations and complications) ought to be obtained and maintained. Even within the case of a earlier laparoscopic strategy, significant adhesions can still be encountered. This is particularly true for the higher belly space (liver and alongside lesser curvature of the stomach), but occasionally even the lower abdomen might be hostile. The presence of international bodies, within the form of rings and meshes, can complicate the laparoscopic approach and delay operative times. Knowledge of the presence of such overseas bodies will assist strategize the reoperation. As beforehand noted, the benefits of laparoscopic restore include shorter hospital stay and quicker recovery, at the expense of longer working instances. In common, both the shortand long-term morbidities, in particular wound infections and hernias, tend to be diminished by the laparoscopic method. Technical Aspects the primary problem in reoperative bariatric surgical procedure consists of accessing the belly cavity. A vital variety of patients have surgical procedure carried out through midline laparotomy and/or repair of an incisional hernia with mesh. We suggest a Hasson approach through the well-healed midline incision or, alternatively, a left higher quadrant Optiview entry. The next step is principally to lyse adhesions to allow recognition of important anatomy. Particularly challenging are the adhesions between the left lobe of the liver and the lesser curvature of the abdomen. Such an anatomical landmark provides the surgeon situational awareness and allows her or him to higher estimate the localization of the vena cava, esophagus, and aorta. This space is usually distorted by the presence of international bodies within the type of anastomotic rings and bands. The presence of a quantity of staple traces and scarred or inflamed tissues predisposes to postoperative ischemia and leaks. It is then necessary to apply several technical modifications, such as increase in staple heights (4. Extensive dissection can result in vascular compromise of the Roux limb, which ought to be totally dissected before beginning the reconstructive a half of the operation. Appropriate handling of thin or probably ischemic tissues might prevent postoperative complications. Because of the identified elevated risk of anastomotic leak after reoperative surgery, routine use of an intraoperative anastomotic leak take a look at should be utilized. The two commonly used strategies include the utilization of methylene blue via a calibration tube and air leak by way of orogastric tube or endoscope. If a optimistic leak check is obtained, the anastomosis should be repaired or redone, and exterior drainage have to be thought-about. If in primary operations a unfavorable intraoperative leak take a look at reduces the incidence of postoperative leak, the predictive value of leak take a look at has not been nicely validated in reoperative surgical procedure. Finally, the advantage of a remnant gastrostomy should be considered in each reoperative case of gastric bypass. The utility of the remnant gastrectomy tube is twofold; it supplies enteral access in case of gastrojejunostomy issues, but also would possibly decrease reoperation for remnant-related problems (functional emptying impairment from vagal damage or distention from distal obstruction). In fact, between 2004 and 2007 the reported cases went from 7 to 23 %, representing a 329 % enhance [7]. Reasons accounting for the rise are the technical ease of the operation, the short hospital keep (commonly even outpatient now), the general low short-term morbidity, the emphasized reversibility, the lower value, and the optimistic weight reduction outcomes, especially in Europe, Australia, and Israel. Common causes for reoperation embody failure of weight reduction and issues, which are categorised as band or port associated (Table 24. Nevertheless, extra parameters, similar to decision of comorbidities and quality of life, should be considered as nicely when defining failures.
Real Experiences: Customer Reviews on Veega
Alima, 50 years: Adipokines are secreted predominantly by adipose tissue, intestine hormones by the gastrointestinal tract and viscera, and cytokines by 16 R. Food then passes by way of the "widespread channel"-the size of jejunum and ileum between the distal anastomosis and the ileocecal valve. This selective aspect of insulin resistance has implications for diabetes, vascular illness, and most cancers. The best predictor of success seems to be genetic similarity amongst related individuals, somewhat than environmental factors [4].
Basir, 31 years: At the end of the 2-year follow-up period, 73 % in the surgical group and thirteen % in the conventional group achieved remission of diabetes (defined as fasting glucose stage <126 mg/dl and glycated hemoglobin [HbA1c] value <6. Throughout the historical past of surgical intervention, surgeons have been keenly thinking about enhancing affected person security, and in nearly each surgical area enhancements have been made. National quality enchancment program analysis of bariatric operations: modifiable danger factors contribute to bariatric surgical opposed outcomes. It is necessary to remember that even when hernia areas have been sutured closed, hernia defects should still type at these sites.
8 of 10 - Review by C. Hogar
Votes: 308 votes
Total customer reviews: 308
